GeriPal - A Geriatrics and Palliative Care Podcast (Alex Smith, Eric Widera)
Explore every episode of GeriPal - A Geriatrics and Palliative Care Podcast
| Pub. Date | Title | Duration | |
|---|---|---|---|
| 01 Aug 2024 | Optimizing Nutrition in Aging: A Podcast with Anna Pleet, Elizabeth Eckstrom, and Emily Johnston | 00:51:42 | |
What is a healthy diet and how much does it really matter that we try to eat one as we age? That’s the topic of this week's podcast with three amazing guests: Anna Pleet, Elizabeth Eckstrom, and Emily Johnston. Emily Johnston is a registered dietitian, nutrition researcher, and Assistant professor at NYU. Anna Pleet is an internal medicine resident at Allegheny Health Network who has a collection of amazing YouTube videos on aging and the Mediterranean diet. Elizabeth Eckstrom is a geriatrician, professor of medicine at OHSU, and author of a new book, the Gift of Aging. I love this podcast as while we talk about the usual topics in a medical podcast, like the role of screening, energy balance, and evidence-based for specific diets, we also talk about what a Mediterranean diet actually looks like on a plate and pepper our guests with questions about their favorite meals to convince Alex and me to eat more like a Sardinian. Eric PS. NEJM just published a great summary of diets summing up adherence to the Mediterranean diet and the following improved health outcomes: death from any cause, cardiovascular diseases, coronary heart disease, myocardial infarction, cancer, neurodegenerative diseases, and diabetes
| |||
| 22 Jul 2021 | Cannabis in Older Adults: A Podcast with Bree Johnston and Ben Han | 00:44:43 | |
Cannabis use by older adults has increased substantially over the last decade, a trend that has paralleled the legalization of its use for medical and recreational purposes. In that same time, there has been a decreased perceived risk associated with cannabis use in older adults as noted in a recent study published in JAGS. On today’s podcast we talk with Drs. Bree Johnston and Ben Han about what the health care providers role is in cannabinoid prescribing and advising when caring for older adults. We try to cover a lot in this podcast, including some of these topics:
| |||
| 05 May 2022 | Hearing Loss in Geriatrics and Palliative Care: A Podcast with Nick Reed and Meg Wallhagen | 00:49:39 | |
Think about the last time you attended a talk on communication skills or goals of care discussions. Was there any mention about the impact that hearing loss has in communication or what we should do about it in clinical practice? I’m guessing not. Now square that with the fact that age-related hearing loss affects about 2/3rd of adults over age 70 years and that self-reported hearing loss increases during the last years of life. Screening for addressing hearing loss should be an integral part of what we do in geriatrics and palliative care, but it often is either a passing thought or completely ignored. On today's podcast, we talk to Nick Reed and Meg Wallhagen about hearing loss in geriatrics and palliative care. Nick is an audiologist, researcher, and Assistant Professor in the Department of Epidemiology at Johns Hopkins Bloomberg School of Public Health. Meg is a researcher and professor of Gerontological Nursing and a Geriatric Nurse Practitioner in the School of Nursing at UCSF. We talk with Nick and Meg about:
If you want to take a deeper dive into this subject and read some of the articles we discussed in the podcast, check out the following:
| |||
| 13 Feb 2025 | Plenary Abstracts at AAHPM/HPNA: Yael Schenker, Na Ouyang, Marie Bakitas | 00:47:19 | |
In today’s podcast we were delighted to be joined by the presenters of the top scientific abstracts for the Annual Assembly of the American Academy of Hospice and Palliative Medicine (AAHPM) and the Hospice and Palliative Medicine Nurses Association (HPNA). Eric and I interviewed these presenters at the meeting on Thursday (before the pub crawl, thankfully). On Saturday, they formally presented their abstracts during the plenary session, followed by a wonderful question and answer session with Hillary Lum doing a terrific job in the role of moderator. Our three guests were Marie Bakitas, who conducted a trial of tele/video palliative care for Black and White inpatients with serious illness hospitalized in the rural south; Yael Shenker, for a trial of patient-directed Prepare-for-your-care vs. facilitated Respecting Choices style advance care planning interventions; and, Na Ouyang, who studied the relationship between prognostic communication and prolonged grief among the parents of children who died from cancer. From just the abstracts we had so many questions. We covered some of our questions on the podcast, others you can ponder on your own or in your journal clubs, including:
Enjoy! -Alex Smith
| |||
| 22 Apr 2021 | Disability in the home: Podcast with Sarah Szanton and Kenny Lam | 00:39:04 | |
We know from study after study that most older adults would prefer to age in place, in their homes, with their families and embedded in their communities. But our health system is in many ways not particularly well set up to help people age in place. Medicare does not routinely require measurement or tracking of disability that leads many people to move out of their homes, and many interventions that support people to age in place are unfunded, underfunded, or funded by philanthropy rather than the government. Today we talk with Sarah Szanton, who created the CAPABLE multi-disciplinary model to help older adults stay at home, and Kenny Lam, who used a national study to examine the need for home-modification devices. And we preview another of the AGS songs for the literature update - this one to the tune of “My Get up and Go” by Pete Seeger. Enjoy! -@AlexSmithMD | |||
| 09 Jun 2022 | Who should get Palliative Care? Kate Courtright | 00:45:20 | |
In the US, geriatrics “grew up” as an academic profession with a heavy research base. This was in part due to the tremendous support of the National Institute on Aging. Clinical growth of geriatrics programs has lagged academic research, despite the rapid aging of the population. Palliative care, in contrast, saw explosive growth in US hospitals. In contrast to geriatrics, the evidence base for palliative care lagged clinical growth, in part because palliative care has no centralized “home” at the National Institutes of Health. The National Palliative Care Research Center (NPCRC)and Palliative Care Research Cooperative (PCRC)were founded in part to meet this need. Today we interview Kate Courtright, a critical care and palliative care physician-researcher who conducts trials of palliative care. Kate’s journey is in a way emblematic of the lack of centralized funding for palliative care: she’s received funding from three separate NIH institutes, the NPCRC, and been involved in the PCRC. We talk with Kate about how despite how far we’ve come in palliative care research, we still don’t have answers to some fundamental questions, such as:
We cover a lot of ground! Working on a mystery. Going wherever it leads. Runnin down a dream… -@AlexSmithMD | |||
| 10 Dec 2020 | Caregiving Boot Camp: Podcast with Zaldy Tan | 00:39:28 | |
“Diagnose and adios.” That’s the sad phrase that I’ve heard quoted more than once, representing caregivers' sentiment of what it’s like to be told by a clinician that your loved one has dementia. This week we talked with Zaldy Tan, Geriatrician and Director of the Memory and Aging program at Cedars Sinai in Los Angeles. With David Reuben at UCLA and others working LA realized that current caregiver training programs were lacking. Caregivers for people with dementia are stressed, short on time, and thirsty for high impact information and skills training that can be delivered efficiently. To meet this need they launched a new caregiver “bootcamp” 1-day training (with the help of Archstone Foundation which also funds GeriPal). We cover many topics, including dissemination of the bootcamp to Spanish-speaking caregivers, converting to video boot camp during COVID, and ways you can partner with them to create your own boot camp. Listen to the podcast to learn more! (And “Remember Me” from Coco - great song choice) JAGS article on caregiver boot camp Dementia caregiver IcareD website (including upcoming bootcamp calendar) CAPC website on caregiver support -@AlexSmithMD | |||
| 24 Mar 2022 | Advance Care Planning Discussion: Susan Hickman, Sean Morrison, Rebecca Sudore, and Bob Arnold | 00:56:34 | |
One of my favorite Piece of My Mind essays in JAMA is by Rebecca Sudore, titled, “Can We Agree to Disagree?” And today our guests agree to disagree. And yet, and yet… They also agree across a whole range of issues, some of which surprised us. This is the latest in our series of podcasts on concerns about, and potential of advance care planning. If you’re new to this discussion, don’t start with this podcast! Start by reading this article by Sean Morrison, Diane Meier, and Bob Arnold in JAMA, and this response from Rebecca Sudore, Susan Hickman, and Anne Walling. Then listen to these prior podcasts with Sean Morrison and Rebecca Sudore about this issue, and we recently discussed differences between Advance Care Planning and Serious Illness Communication with Juliet Jacobsen and Rachelle Bernacki. On today’s podcast we ask our guests about areas in which there might be agreement or disagreement, including:
Among other topics. I’m heartened that we could have this discussion as a field, as it shows that we’ve grown to the point where we can agree to disagree respectfully with each other. We can work it out! Links to a few couple items mentioned on the podcast: -@AlexSmithMD | |||
| 11 Apr 2024 | Ambivalence in Decision-Making: A Podcast with Joshua Briscoe, Bryanna Moore, Jennifer Blumenthal-Barby & Olubukunola Dwyer | 00:51:34 | |
Ambivalence is a tough concept when it comes to decision-making. On the one hand, when people have ambivalence but haven't explored why they are ambivalent, they are prone to bad, value-incongruent decisions. On the other hand, acknowledging and exploring ambivalence may lead to better, more ethical, and less biased decisions. On today's podcast, Joshua Briscoe, Bryanna Moore, Jennifer Blumenthal-Barby, and Olubukunola Dwyer discuss the challenges of ambivalence and ways to address them. This podcast was initially sparked by Josh’s “Note From a Family Meeting” Substack post titled “Ambivalence in Clinical Decision-Making,” which discussed Bryanna’s and Jenny’s 2022 article titled “Two Minds, One Patient: Clearing up Confusion About Ambivalence." Bryanna’s and Jenny’s article is particularly unique as it discusses these “ambivalent-related phenomena” and that these different kinds of “ambivalence” may call for different approaches with patients, surrogates (and health care providers): In addition to defining these “ambivalent related phenomena” we ask our guests to cover some of these topics:
Lastly, the one takeaway point from this podcast is that the next time I see ambiguity (or have it myself), I should ask the following question: “I see you are struggling with this decision. Tell me how you are feeling about it.”
| |||
| 06 Oct 2022 | Evidence-Based Messaging for Serious Illness Care: A Podcast with Tony Back and Marian Grant | 00:50:37 | |
Earlier this year palliative care was the correct response to the following clue on the game show Jeopardy:
What struck me most was not that palliative care was a question, nor that it made it seem that palliative care isn’t provided alongside care directed at curing, nor was it that hospice was the first buzzed in response, but it was that palliative care was the $2000 question in the Double Jeopardy round! The fact that palliative care was the hardest of questions told me that we have a massive messaging problem in our field. So what do we do about it? Well, on today’s podcast we talk with Marian Grant and Tony Back, who with support form the John A Hartford Foundation and the Cambia Health Foundation, have done a deep dive into the research on layperson perceptions of palliative care, hospice, and advance care planning. The result is a new toolkit to help us fix our messaging & engage the public: seriousillnessmessaging.org Questions we talk about include:
Public Perceptions of Advance Care Planning, Palliative Care, and Hospice: A Scoping Review Public Messaging for Serious Illness Care in the Age of Coronavirus Disease: Cutting through Misconceptions, Mixed Feelings, and Distrust Effective Messaging Strategies: A Review of the Evidence. Communicating to Advance the Public's Health: Workshop Summary
| |||
| 09 May 2024 | Public Facing Education via Social Media: A Podcast with Julie McFadden, Matt Tyler, Sammy Winemaker and Hsien Seow | 00:47:51 | |
On today’s podcast, we’ve invited four hospice and palliative care social media influencers (yes, that’s a thing!), all of whom focus their efforts on educating the general public about living and dying with a serious illness. Their work is pretty impressive in both reach (some of their posts are seen by millions of viewers) and breadth of work. We’ve invited:
So, take a listen and check out their social media sites to get inspired. Just don't let Alex make me do another TikTok dance…
Eric Widera
| |||
| 03 Feb 2022 | Structural, Institutional, and Interpersonal Racism: Podcast with Deborah Ejem and Deep Ashana | 00:48:33 | |
In prior podcasts we talked about racism and COVID, lack of diversity in the palliative care workforce, racial and ethnic differences in end of life care, and implicit bias in geriatrics and palliative care. Today our focus is on structural, institutional, and interpersonal racism, and how these different but related constructs negatively impact the care of older adults and people with serious illness. We are joined by Deborah Ejem, a medical sociologist and Assistant Professor in the School of Nursing at the University of Alabama Birmingham, and Deep Ashana, a pulmonary critical care physician and Assistant Professor of Medicine at Duke University. We discuss:
We could have continued talking with our guests for hours. We will continue to address the issue of racism in future podcasts. -@AlexSmithMD | |||
| 15 Apr 2021 | All things Amyloid, including Aducanumab and Amyloid PET scans with Gil Rabinovici | 00:53:10 | |
There are no currently approved disease modifying drugs for Alzheimer's disease, but in a couple months that may change. In July of 2021, the FDA will consider approval of a human monoclonal antibody called Aducanumab for the treatment of Alzheimer's disease. If approved, it will not only make this drug the defacto standard of care for Alzheimer's disease, but will create a monumental shift in the usage of other currently limited diagnostic tests, including Amyloid PET scans and other biomarkers. On today's podcast, we talk about all things Amyloid, including Aducanumab and Amyloid PET scans with Gil Rabinovici. Dr. Rabinovici is the Edward Fein and Pearl Landrith Endowed Professor in Memory & Aging at UCSF. I could talk to Gil all day long, but we try to fit all of these topics in this jam-packed podcast:
| |||
| 18 Mar 2021 | Expelled from Hospice: Podcast with Elizabeth Luth and Lauren Hunt | 00:38:21 | |
Hospice may not be a great match for all of the care needs of people with dementia, but it sure does help. And, as often happens, when patients with dementia do not decline as expected, they are too frequently discharged from hospice, an experience that Lauren Hunt and Krista Harrison refer to in an editorial in the Journal of the American Geriatrics Society (JAGS) as feeling like being “expelled.” We talk on this week’s podcast with Elizabeth Luth, author of a study in JAGS about her study of patients in a large New York Hospice with dementia who either are discharged from hospice or live longer than 6 months. Turns out this happens - brace yourselves - nearly 40% of the time! And we talk with Elizabeth and Lauren Hunt, who helps us contextualize these findings in the setting of larger issues around the fit of hospice for persons with dementia and hospice Medicare policy. (We will add the link to the editorial when it’s uploaded to the JAGS website). -@AlexSmithMD | |||
| 12 Jan 2023 | Improving Hospital Care for Older Adults through Acute Care for Elders (ACE Units): A Podcast with Kellie Flood and Stephanie Rogers | 00:47:44 | |
Acute Care for Elders (ACE Units) have been around for over a quarter of a century. Randomized trials of ACE units date back to 1996 when Seth Landefeld and colleagues published a study in NEJM showing that they improve basic activities of daily living at discharge and can reduce the frequency of discharge to long-term care institutions. But if ACE units are so great, why do so few hospitals have them? On today's podcast we talk about ACE units with geriatricians Kellie Flood and Stephanie Rogers. They recently published a paper in JAGS looking at the current landscape of ACE units in the US. In the podcast we go over these issues and more:
If you want to do a deeper dive in ACE units, check out some of the following articles:
| |||
| 08 Aug 2024 | Between Two Urns: Undertaker Thomas Lynch | 00:47:34 | |
(We couldn’t resist when Miguel Paniagua proposed this podcast idea and title. And no, you’ll be relieved to hear Eric and I did not imitate the interview style of Zach Galifiniakis). We’ve talked a good deal on this podcast about what happens before death, today we talk about what happens after. Our guest today is Thomas Lynch, a poet and undertaker who practiced for years in a small town in Michigan. I first met Thomas when he visited UC Berkeley in the late 90’s after publishing his book, “The Undertaking: Stories from the Dismal Trade.” We cover a wide range on this topic, weaving in our own stories of loss with Thomas’s experiences, stories, and poems from years of caring for families after their loved one’s have died. We cover:
| |||
| 27 Apr 2023 | GeriPal Special: Hopes and Worries for Hospice and Palliative Care | 00:11:29 | |
We have a special extra podcast this week. During the last AAHPM - HPNA meeting in Montréal, we went around asking attendees what one thing that they are most worried about and one thing they are most hopeful for when thinking about the future of our field. We couldn’t fit everyone’s responses in but came up with the big themes for questions and edited them into this weeks podcast / YouTube video. Eric and Alex
DISCLAIMER While we filmed in Montreal during the Annual Assembly, all opinions expressed in this podcast are independent of AAHPM and HPNA, or the Annual Assembly. Furthermore, direction to external websites is not an endorsement from AAHPM or HPNA, or the Annual Assembly.
AccentCare, a portfolio company of private equity firm Advent International, is another example. The company has expanded its palliative care services through partnerships with hospitals and other managed care providers, according to AccentCare CEO Stephan Rodgers. “We’ve got a very large palliative care practice,” Rodgers told PCN. “What we’ve seen to make it really work is you either have to be in the hospital, where we’ve taken over palliative care in the hospital, or you have to be contracted with managed care and get it at some kind of risk, because community-based palliative care is very difficult to make operate right now from a profitable [perspective].”
| |||
| 11 Jan 2024 | What is going on with MAID in Canada? Bill Gardner, Leonie Herx, & Sonu Gaind | 00:52:45 | |
Four percent of deaths in Canada are due to Medical Assistance in Dying (MAID). Four percent. The number of people who have used MAID in Canada since it was legalized in 2016 has increased year on year from about 1,000 people in the first year to over 13,000 people in 2022. California, which has a similar population size as Canada and legalized MAID around the same time, has fewer than 1000 deaths per year from MAID. In further contrast to the United States, MAID in Canada is almost entirely administered by a clinician, whereas in the United States patients must self administer. To be eligible in Canada patients must have a “grievous and irremediable” condition, including disability; they do not have to have a terminal illness with a prognosis of less than 6 months. They could have a prognosis of years, or decades. A planned expansion of MAID to include people with mental illness was placed on hold until March 2024. The Canadian parliament will soon hear a report on potentially expanding MAID to “mature minors.” A recent Human Rights podcast discussed the story of a Canadian seeking MAID because he could not afford to stay housed. Today we talk about these issues with Bill Gardner, a psychologist at the University of Ottawa who is living with cancer, Leonie Herx, a palliative care physician at the University of Calgary, and Sonu Gand, a psychiatrist at the University of Toronto and former president of the Canadian Psychiatric Association. We talk about how Canada got to this point, including the degree to which offering MAID to anyone who is eligible has become standard practice in many places. We hear Bill Gardner's experience being told that his cancer could not be treated and immediately offered two options: palliative care or MAID. We talk about the role of palliative care and lack of access for many people living with serious illness in Canada. We go in depth about ethical issues raised by the planned expansion of MAID to people with mental illness. Much of the criticism of the explosion of MAID in Canada is coming from people like, our guests, who feel that MAID should be an option for a select few, rather than coming from under-no-circumstance opponents. To many this rapid expansion will represent autonomy run amok. It is the slippery slope made real. To others MAID represents a seemingly easy and inexpensive mechanism to address failures of the system to address potentially reversible sources of suffering on a systemic level, from difficult conversations at the bedside, to meeting basic needs like housing. For those listening to the podcast, credit to Kai for guitar on Neil Young’s Cortez the Killer (my left hand is still broken at the time of this recording). You get me with one-finger-chords on the guitar if you're watching on YouTube (best I could manage). -@AlexSmithMD Bill Gardner’s article about MAID in Comment Magazine Bill Gardner’s articles about living with terminal cancer in Mockingbird Magazine:
| |||
| 16 Dec 2021 | Geriatric Oncology: Podcast with Melisa Wong and Louise Walter | 00:44:47 | |
Geriatric Oncology has arrived. Yes, Louise Walter has been leading the fight to improve cancer screening in older adults for years. But when it came to geriatricizing the way we assess and treat older adults with cancer, the evidence was thin. In our prior podcast with Supriya Mohile and William Dale on geriatric assessment in oncology, we couldn’t say for certain if a geriatric assessment was helpful for patients with cancer. Well now we can. We are joined by Melisa Wong, a geriatric oncologist, and Louise Walter, a geriatrician and leader in cancer screening for older adults, to talk about the shifting landscape of geriatric oncology, including:
Links of Interest: And as a bonus, you get to hear Louise on piano and vocals and I cover Wouldn’t It be Loverly, from My Fair Lady. -Enjoy! | |||
| 13 Nov 2020 | Age Friendly Health Systems: Podcast with Julia Adler-Milstein and Stephanie Rogers | 00:40:02 | |
An age friendly health system is one in which everyone, from the doctors to the nurses to the people cleaning the rooms are aware of the unique needs of older adults. These needs are categorized around the 4 M’s - Medication, Mentation, Mobility, and What Matters Most. But we cannot achieve the ideal of an age friendly health system without, well, changing systems. In this week’s podcast, we talk with Julia Adler- Milstein about the ways in which the electronic health records in hospitals and skilled nursing facilities are set up (or not set up) to document and track the 4 M’s. We also talk with Stephanie Rogers about her work toward creating an age friendly health system at UCSF. Enjoy! -@AlexSmithMD | |||
| 21 Apr 2022 | Poetry & Palliative Care: Podcast with Mike Rabow and Redwing Keyssar | 00:44:56 | |
In celebration of National Poetry Month, we are delighted to share with you the second podcast in our series on poetry and medicine. In the first podcast, we talked with Guy Micco and Marilyn MacEntyre about poetry and aging. In this second part in our series, we welcome Mike Rabow and Redwing Keyssar to talk about palliative care and poetry. As with aging, poetry operates on multiple levels within the palliative care space. Poetry puts us in our patient’s shoes. As Redwing’s poem says, “why not live as long as possible?” Poetry holds us in that liminal space so many of our patients are in. Paradox. The impossiblity which is life, which is everything, and death, which is the end of life. As Mary Oliver tells us In Blackwater Woods, and I’m paraphrasing here, we must to hold it to our bones, knowing our lives depend on it, and when the time comes, to let it go. To let it go. Or as in Mark Nepo’s poem Adrift, I am so sad and everything is beautiful. Poetry helps us grapple with our own experiences of illness. Redwing, who is a cancer survivor, shares poems about her experiences with cancer. Mike Rabow shares his award winning poem about coming out to the world about his diagnosis with multiple sclerosis. We talk not only about reading poetry, but also writing poetry, and using poetry in medical education as a healing modality. And along the way, we really felt like we got to the heart of things. To the deeper emotions - of loss and grief, of wonder and transcendence - that are at the heart of the complex care we provide. -@AlexSmithMD
Food for Thought Poetry for Resiliency Loss, Losing and Loosening, poetry for grief and loss Wounded Healer poetry sessions
Mike Rabow’s Comprehensive Care Team randomized trial of outpatient palliative care
In addition to Redwing’s own songs and poems, other poems read by Mike and Redwing during the podcast: In Blackwater Woods by Mary Oliver Talk Before Sleep by Elizabeth Berg Late Fragment by Raymond Carver
| |||
| 02 Feb 2023 | Books on Becoming A Better Mentor (and Better Person): Bob Arnold | 00:49:43 | |
Sometimes you read a book and get a flash of insight - that “ah ha!” moment - about yourself and the ways you interact with others. That happened to me when reading “Range: Why Generalists Triumph in a Specialized World.” It helped me to understand and justify my interest in (this won’t surprise you) EVERYTHING related to geriatrics or palliative care. Also hat tip to Matthew Growdon for recommending the book. Today we talk with Bob Arnold, who has a long list of recommendations for books that have the potential to generate an “ah ha!” moment. The podcast is ostensibly focused on becoming a better mentor, but as you’ll hear, we discuss techniques that can help you cope with anxiety, stress, your spouse…the list goes on. In reality, insights from these books can help you be a better teacher, a more curious person, as well as a better mentor or mentee. Bob urges you to buy these books from your local bookstore. To that end, we’re not including links with the titles below. Please shop locally. As a bonus, Lauren Hunt, frequent guest on GeriPal, heard we recorded this podcast and wanted to add a couple books to Bob’s list (she saw Bob give a talk about these books at the NPCRC Foley retreat). Her list will strongly resonate with women in academics. See below for Lauren’s two additions to Bob’s list, with her personal commentary. Enjoy! -@AlexSmithMD
Bob’s booklist:
From Lauren: The Secret Thoughts of Successful Women: Why Capable People Suffer from the Impostor Syndrome and How to Thrive in Spite of It by Valerie Young I was inspired to read this book after reading a post on the 80,000 hours blog. I had heard of course heard of imposter syndrome in the past but I didn’t make the connection to myself until I read this article and saw my thoughts printed on the page. You would think that after several years of a number of career successes, the imposter syndrome would have abated for me, but rather I found it getting worse! I thought that I should know more of what I was doing by this point in my career, but instead I often felt like I had no idea what I was doing! So I came across this book and found it very helpful. Young defines people who have imposter syndrome as those who have a “persistent belief in their lack of intelligence, skills, or competence. They are convinced that other people’s praise and recognition of their accomplishments is undeserved, chalking up their achievements to chance, charm, connections, and external factors. Unable to internalize or feel deserving of their success, they continually doubt their ability to repeat past successes.” I certainly related to the point that instead of successes alleviating feelings of fraudulence, the opposite happens, because it increases pressures to uphold one’s reputation. The pressures can be intense, leaving one wondering if it’s all worth it, and prompting fantasies of leaving the charade behind. One thing I really liked about this book is that it places the imposter syndrome into the context of a patriarchal, misogynistic, racist society and organizations that create cultures that cultivate self-doubt (ahem academia). Imposter syndrome is a rationale response to a crazy world. We exist in a society and culture that actually judges women to be less competent at work (the studies she details are SUPER disturbing). It is not surprising we would internalize these norms. Also that being underrepresented in a field creates pressures not only to represent just oneself, but an entire gender. She focuses on women, but these concepts obviously apply to people of color and other disadvantaged social groups. And of course men can have imposter syndrome too. Another part I liked about the book is digging into the notion that one’s success is due to luck, or being in the right place at the right time. She dispels these notions by pointing out that, first of all, luck is always present, even for people who are enormously talented and second, being the right place at the right time, having the right connections, and having a winning personality can sometimes actually be the result of skills or abilities, often the result of hard-work, hustling, and efforts to develop one’s socioemotional capacity. This is a self-help book, so throughout she offers some useful rules and self-talk for responding to imposter syndrome thoughts. She details different ways to respond to thoughts based on your competence type. For example, if you are a perfectionist, she recommends reframing to a “good enough” quality standard—a mantra I adopted from colleague during the pandemic and has been incredibly helpful for me over the past few years. For the rugged individualist who equate true competence equals solo, unaided achievement, the reframe is “competence means knowing how to identify the resources needed to get the job done.” Another really important idea she raises is that women often have difficult choices to make about their career and its impact on other parts of their families and their other social networks that aren’t as pronounced for men in our society. Sometimes it is difficult to disentangle these questions from feelings of imposter syndrome. For example, is reluctance to take on more responsibility at work or relocate because you feel inadequate or is it because of genuine concern about the impact on your family? Moreover, women (generalizing here) tend to place lower value on traditional measures of work success (e.g. money, power, influence) and greater value on connection and meaning. It can require a lot of soul searching to figure out whether one is avoiding career “success” out of fear or that certain paths are just truly not aligned with our values. Finally, towards the end of the book, she introduces the idea of “faking it till you make it” and having chutzpah—i.e going for it. Of course, she’s not advocating for a George Santos approach (no lying) but just having a little bit more of a mindset that you’ll figure it out once you’re on the job. I’d definitely recommend this book if you’ve ever struggled with similar feelings or mentor people who might. She’s got a breezy and relatable writing style that’s easy to read, lots of great real-world stories, and piquant quotes.
The No Club: Putting a Stop to Women’s Dead-End Work by Linda Babcock, Brenda Peyser, Lise Vesterlund, and Laurie Weingart Summary of the book’s premise:
Before I read this book, I didn’t fully grasp the idea that an activity would be helpful to the organization but not to my own career. Sometimes requests for participation in these activities come with a veneer or prestige and lots of feel-good gratitude. I personally feel a lot of guilt and worry about disappointing people when I say no to things. Even declining to review an article for a journal is accompanied by some stomach knots (it’s so hard to find reviewers!) I also place a lot of value in collaboration and working in teams, and the idea of working in a culture where everyone is only looking out for themselves is not appealing to me. But I’m also worried at the level of overwhelm I experience at times and perhaps some of you have experienced as well. How do we ensure that we are on sustainable path where we can stay in and build the world we want to live and work in? The book also got me thinking about what is promotable or not in academia, i.e. what is the currency. I think we all know that grants and publications are promotable activities, but even within that there are hierarchies. Some of these hierarchies I think I understand: a data-based paper in a high-impact journal has higher promotability than an editorial in a lower-impact journal. Some of them I’m not sure about: is an NIH project grant more promotable than a foundation grant and if so why (bc higher indirects?) Also, things like mentorship seem gray to me: senior-authored articles are evidence of independence and potential track to mentoring awards, but people often seem to place mentorship in the NPT category. I think having more transparency and discussion about what is promotable or not would be very useful. Highly recommend this book for women, men, people in leadership, and employees. It’s extremely well-written, nuanced, and eye-opening.
SPONSOR: This episode of the GeriPal Podcast is sponsored by UCSF’s Division of Palliative Medicine, an amazing group doing world class palliative care. They are looking for physician faculty to join them in the inpatient and outpatient setting. To learn more about job opportunities, please click here: https://palliativemedicine.ucsf.edu/job-openings
| |||
| 02 Feb 2024 | RCT of Default Inpatient PC Consults: Kate Courtright & Scott Halpern | 00:47:19 | |
Last week we talked about a trial of a nurse and social worker outpatient palliative care intervention published in JAMA. This week, we talk about the other major palliative care trial of default palliative care consults for hospitalized older adults with COPD, kidney disease, or dementia, published in the same issue of JAMA. (See also our accompanying editorial, first author Ashwin Kotwal who joins today as a co-host, and a podcast I recorded with JAMA editor Preeti Malani). For context, listen to the prior podcast with Scott on “nudges” and prior podcast with Kate on who should get palliative care. Three things I love about this podcast, and why you should listen. First, in our editorial, we expressed concern about the length of stay metric not being patient centric, though important for health systems focused on cost savings. It was refreshing to hear Scott and Kate express similar sentiments. Second, we wanted to know how the palliative care clinicians felt about the increased workload - and we had some glimpses into those experiences (and hope for a future publication that fleshes it out further). Finally, we heard about next steps and lessons learned, as though this was the largest pragmatic trial of palliative care to date, it isn’t their last. Much more to come. And next time maybe we really will play the game where every time the word pragmatic is mentioned you have to drink 🙂 And I get to play Phish, who Scott has seen about 100 times in concert. I saw them only twice. Once as an undergraduate at Michigan, in 1994. They played Hill auditorium and I signed up to be an usher. Can you imagine trying to usher Phish Heads to stay in their assigned seats? Yeah, no. Gave up at some point and joined them. Full electric experience. Second time was with Neil Young at the Bridge School Benefit at the Shoreline Amphitheater, California in 1998. That concert, entirely acoustic, was impressive in its sheer musical virtuosity. You're kind of naked playing acoustic like that. On today’s podcast you get me, not naked, though still only with 2 left fingers (hand still broken) on the guitar, playing “Miss You.” -@AlexSmithMD
Additional links: Trey Anasatsio playing Miss You alone and acoustic, start around 21 minutes for the lead in Original article describing the potential for default options to improve health care delivery: https://www.nejm.org/doi/full/10.1056/NEJMsb071595 Scott on goals of care as the elusive holy grail outcome of palliative care trials (we discussed toward the end): https://www.nejm.org/doi/full/10.1056/NEJMp1908153 The protocol paper for REDAPS: https://www.atsjournals.org/doi/10.1513/AnnalsATS.201604-308OT Big recently funded PCORI trial comparing specialist PC delivered by default vs. generalist PC following CAPC training + a different EHR nudge: https://www.pcori.org/research-results/2023/comparative-effectiveness-generalist-versus-specialist-palliative-care-inpatients Kate’s “Palliative Connect” RCT: https://clinicaltrials.gov/study/NCT05502861?term=katherine%20courtright&rank=1
| |||
| 29 Dec 2022 | Negotiation and Dispute Resolution: A Podcast with Lee Lindquist and Alaine Murawski | 00:50:11 | |
From discussing “taking away the keys to the car” for a cognitively impaired older adult to decisions to limit life sustaining treatments at the end of life, conflict and disagreement permeate everything that we do in medicine. How well though are we taught to handle conflict and disagreement? I’d say not well as I don’t think I’ve ever received a formal talk on the issue. On today’s podcast we take a deep dive into the topic of Negotiation and Dispute Resolution training with Lee Lindquist and Alaine Murawski. We’ve had Lee on before to talk about her Plan your Lifespan project. We invited her back along with Alaine to talk about their work around negotiation training, including their work on NegotiAge, an online, AI based training intervention designed to teach negotiation skills to caregivers. For an ever deeper dive into the subject of negotiation and dispute resolution, check out the following links (and for any caregivers interested in participating in the randomized clinical trial of the NegotiAge training, feel free email the NegotiAge Research Team at negotiage@northwestern.edu):
| |||
| 29 Apr 2021 | Life, Death, and a Hospital Strained by COVID: Podcast with Brian Block, Sunita Puri and Denise Barchas | 00:42:17 | |
During the winter peak in coronavirus cases, things got busy in my hospital, but nothing close to what happened in places like New York City last spring or Los Angeles this winter. Hospitals in these places went way past their capacity, but did this strain on the system lead to worse outcomes? Absolutely. On today’s podcast, we talk with Brian Block, lead author of a Journal of Hospital Medicine study that showed that patients with COVID-19 admitted to hospitals with larger COVID-19 patient surges had an increased odds of death. We talk about the findings in his study, which also included some variation in the surge hospitals as well as potential reasons behind these outcomes. We’ve also invited two other guests, Denise Barchas and Sunita Puri, to describe their hospital experiences in a COVID surge. Denise is a ICU nurse at UCSF who volunteered in New York during the spring surge of COVID cases. Sunita is the Medical Director of Palliative Medicine at USC’s Keck Hospital & Norris Cancer Center in Los Angeles. She is also the author of numerous books and essays, including “That Good Night: Life and Medicine in the Eleventh Hour” (if you haven't read it yet you should!)
| |||
| 05 Dec 2024 | Stories We Tell Each Other to Heal: Ricky Leiter, Alexis Drutchas, & Emily Silverman | 00:48:34 | |
We’ve covered stories before. With Liz Salmi, Anne Kelly, and Preeti Malani we talked about stories written up in the academic literature, such as the JAMA Piece of My Mind series. We talked with Thor Ringler, who helped found the My Life My Story Project at the VA and beyond, and Heather Coats about the evidence base for capturing patient stories. Today’s podcast is both similar and different. Similar in that the underlying theme of the power of stories. Different in that these storytelling initiatives, the Nocturnists and the Palliative Story Exchange, are focused on clinicians sharing stories with each other in small groups to heal. There’s something magical that happens in small group storytelling. It’s that mixture of intimacy and vulnerability, of shared clinical experiences, that fosters a sense of belonging. We model that small group storytelling experience today. We discuss:
These initiatives arose organically from clinicians as part of a journey away from burnout, moral distress, shame, and loneliness toward healing, wholeness, gratitude, and belonging. A journey taken one story at a time. One final note on the song request: About 20 years ago I took an epidemiology course as part of a Masters program. The instructor, Fran Cook, gave all the students a survey without explanation. We answered the survey and handed it in. One of the questions was, “Can you name a song by the Tragically Hip?” It later turned out the survey was a prognostic index designed to determine if the respondent was Canadian.
| |||
| 19 Dec 2024 | Palliative Care for Mental Illness: A Podcast with Dani Chammas and Brent Kious | 00:49:44 | |
We’ve talked a lot before about integrating psychiatry into palliative care (see here and here for two examples). Still, we haven’t talked about integrating palliative care into psychiatry or in the care of those with severe mental illness. On this week’s podcast, we talk with two experts about palliative psychiatry. We invited Dani Chammas, a palliative care physician and psychiatrist at UCSF (and a frequent guest to the GeriPal podcast), as well as Brent Kious, a psychiatrist at the Huntsman Mental Health Institute, focusing on the management of severe persistent mental illnesses. We discuss the following:
Here are a couple of articles if you want to do a deeper dive:
| |||
| 24 Jun 2021 | Neuropalliative Care: A podcast with Benzi Kluger, Edward Richfield, and Christine Ritchie | 00:43:13 | |
While palliative care most traditionally grew up with a strong association with cancer care and end-of-life care, more and more evidence is coming out about how to integrate palliative care into a variety of serious illnesses from heart failure to chronic lung conditions. Another emerging field is the integration of neurology and palliative care, something that has been coined as “neuropalliative care.” We had Benzi on a previous GeriPal podcast to talk about palliative care in Parkinson's disease. On this week’s podcast we go much deeper into the field of neuropalliative care by inviting leaders of the new field and in the International Neuropalliative Care Society (INPCS), Benzi Kluger, Edward Richfield, and Christine Ritchie. INPCS connects clinicians, researchers, interdisciplinary team members, people living with neurological illness, family members, and advocates at the intersection of neurology and palliative care. In addition to talking about why INPCS was developed, we talk with these leaders about:
One other big shout out too for INPCS is for their inaugural Annual Meeting on November 4-6, 2021. The online conference will offer attendees the opportunity to learn from experts, hear updates in practice patterns, review the state of the science in neuropalliative care, and network with others interested in this growing field. Best part, it’s free! So sign up. | |||
| 20 Mar 2025 | Hastening Death by Stopping Eating and Drinking: Hope Wechkin, Thaddeus Pope, & Josh Briscoe | 00:51:26 | |
Eric and Alex have featured discussions about complex bioethical concepts around caring for people at the end of life, including voluntarily stopping eating and drinking (VSED), and multiple episodes about the ethical issues surrounding medical aid in dying (MAID). Recently, discussion has emerged about how these issues intertwine in caring for patients with advancing dementia who have stated that they would not want to continue living in that condition: for those with an advanced directive to stop eating and drinking, how do we balance caring for their rational past self and their experiential current self? Should these patients qualify for medical aid in dying medications? And is there a middle path to provide some degree of comfort while also hastening the end of life? To delve into these questions, we spoke with Hope Wechkin, medical director of EvergreenHealth home hospice, who authored an article describing a process of Minimal Comfort Feeding (MCF) for patients who have expressed an interest in not wanting to live with advanced dementia. MCF, which Hope implemented for one of her hospice patients, serves as a middle way between the discomfort to the patient and caregivers of completely withholding food and fluid, and the current practice of comfort feeding only in which food and fluid are routinely offered to patients even in the absence of a symptomatic benefit. We were also joined by Thaddeus Pope, JD and Dr. Joshua Briscoe, to discuss the topic of voluntarily stopping eating and drinking as a potential bridge to access medical aid in dying medications and their respective articles on the topic. We discussed what makes an illness “terminal”, what goes into assessing capacity for an action as simple as requesting something to drink, and whether the TV show Severance illuminates any of these answers. -Theo Slomoff, UCSF Palliative Care Fellow 2024-25 (guest host)
Past GeriPal Podcast Episodes on MAID: MAID podcasts https://geripal.org/what-is-going-on-with-maid-in-canada-bill-gardner-leonie-herx-sonu-gaind/ https://geripal.org/assisted-dying-podcast-with-lewis-cohen/ https://geripal.org/dilemmas-in-aid-in-dying-podcast-with/
Past GeriPal Podcast Episode about VSED: https://geripal.org/tim-quill-vsed/
| |||
| 29 Jan 2021 | LGBT Care for Older Adults and Serious Illness: Podcast with Carey Candrian and Angela Primbas | 00:38:22 | |
Lesbian, gay, bisexual and transgender (LGBT) older adults have lived through a lifetime of discrimination, social stigma, prejudice, and marginalization. Is the care that we are giving them in later life changing any of that or are we pushing them back into the closet? This is what we talk about in this week's podcast with Carey Candrian from the University of Colorado School of Medicine, and Angela Primbas from Stanford University (and future geriatrics fellow at UCSF!). Carey has published a wonderful article in the Gerontologist titled “She’s Dying and I Can’t Say We’re Married?”: End-of-Life Care for LGBT Older Adults, in which she describes how older LGBT adults may be at higher risk for having their health care wishes ignored or disregarded, their families of choice are less likely to be included in their decision making, and they may experience increased isolation, bullying, mistreatment, or abuse, which ultimately contribute to receipt of poor-quality health care. We talk about the scripts that we use in medicine that may hamper open discussions about sexual orientation and gender identity (SOGI) including the term “family meeting”, the need to revise our intake forms to incorporate SOGI questions, and the need for education. We also get a chance to hear Alex Sing “The Story” whose lyrics very much speak to the subject at hand: “All of these lines across my face If you want to learn more, please check out these wonderful resources:
| |||
| 27 Oct 2022 | New Prognostic Models for Older Adults: Alex Lee, James Deardorff, Sei Lee | 00:47:15 | |
Dr. Faith Fitzgerald once quipped that prognostic modeling is the “punctilious quantification of the amorphous.” She has a point. Prognosis is inherently uncertain. As Alex Lee says on our podcast today, all prognostic models will be wrong (in some circumstances and for some patients); our job is to make prognostic models that are clinically useful. As Sei Lee notes, the argument for developing prognostic models has won the day, and we increasingly use prognostic scores in clinical decision making. What makes prognostic models for mortality different from models used for anticoagulation or risk of renal injury? James Deardorff replies that there is something inherently different about predicting mortality. Death is different. For some reason clinicians who might be perfectly comfortable using an anticoagulation risk calculator might be skeptical of a mortality risk calculator (see this recent terrific JAMA IM study from Nancy Shoenborn on this issue). And yet, the only thing that may be worse than a prognostic calculator is a clinician relying solely on their clinical intuition. Today our guests Alex Lee, James Deardorff, and Sei Lee, talk to us about the uses, limitations, and clinical use cases for prognostic models. As a springboard for this conversation we discuss new prognostic models developed to predict (simultaneously) mortality, disability, and mobility impairment (Alex Lee first author, JAGS) and mortality for people with dementia residing in the community (James Deardorff first author, JAMA IM). Both new models are now available and free to use on ePrognosis. And Sei and Eric reminisce about slow dancing to “Forever Young” by Alphaville in their teenage years. Enjoy! -AlexSmithMD | |||
| 15 Sep 2022 | Aortic Stenosis, TAVRs, and Code Status: A Podcast with Gwen Bernacki and Ashok Krishnaswami | 00:47:14 | |
Transcatheter aortic valve replacement (TAVR) has revolutionized the treatment of valvular heart disease for patients with severe aortic stenosis, a condition that affects one in ten adults older than the age of 80. The rates of TAVR have also risen dramatically in the last decade. In 2019, the number of TAVRs exceeded surgical aortic valve replacement (SAVR) in the US for the first time. On today’s podcast we talk with two amazing cardiologists and researchers - Gwen Bernacki and Ashok Krishnaswami - about TAVRs in the elderly, including what it is, who gets it, and what the outcomes and complications look like after the procedure. We also discuss Gwen and Ashok’s mixed-method study in the Journal of the American Geriatrics Society (JAGS) where they interviewed TAVR coordinators across California and Washington State about how code status is managed within their programs, and compared programs according to their policies to assess differences in outcomes. What they found was fascinating:
Gwen and Ashok want to make it clear how thoughtful interventionists are about this topic for their patients — as this is very very challenging on a daily basis for them. They also advocate for having more great minds at the table to help move the field forward (including geriatric and palliative care specialists!) Here are more resources if you want to take a deeper dive into the subject:
| |||
| 30 Mar 2023 | Storytelling in Medicine: A Podcast with Liz Salmi, Anne Kelly, and Preeti Malani | 00:50:03 | |
Two weeks ago on the GeriPal podcast we talked about why and how to write for the general public. This week we’ve invited three guests to share their stories about storytelling that’s written for healthcare providers. The first guest is Liz Salmi. Liz wrote a fabulous perspectives piece in the NEJM titled “Deciding on My Dimples” which talks about her experience as a patient doing shared decision making during neurosurgery for resection of an astrocytoma. In addition to this being a fascinating story, Liz brings in a great perspective as a patient, advocate, researcher, and a punk rocker. Our second guest is a recurring star of GeriPal, Anne Kelly. She just published an essay for JAMA Piece of My Mind titled “The Last Visit”. In this piece Anne describes her experience with the expressions of love she and her mother shared in the last days of her mothers life. Lastly, but certainly not least, we’ve invited Preeti Malani. Preeti is the editor for JAMA’s Piece of My Mind section. We’ve asked Preeti to come on to describe what happens behind the curtain when evaluating these stories, including what makes those few that get accepted stand out. We’ve also love to hear from you on twitter and facebook your own experiences writing for the medical world (and please include links!) | |||
| 24 Feb 2022 | Should We Shift from Advance Care Planning to Serious Illness Communication? | 00:49:02 | |
There is a lively debate going on in academic circles about the value of Advance Care Planning (ACP). It’s not a new debate but has gathered steam at least in palliative care circles since Sean Morrisons published a JPM article titled “Advance Directives/Care Planning: Clear, Simple, and Wrong.” Since then there has been a lot of back and forth, with even a couple of podcasts from us, several JAMA viewpoints, and most recently a series of published replies from leaders in the field on why ACP is still valuable (see below for references). Despite all of these publications, I’m still left at a loss of what to think about it all. Most of the debate seems rather wonky, as honestly it feels like we are getting stuck in the weeds of semantics and definitions, like what counts as ACP versus in the moment decisions. But the consequences are real, from research funding dollars to health systems investment. So in today's podcast, we have invited Juliet Jacobsen and Rachelle Bernacki to talk about what all the fuss is about. Juliet and Rachelle are two of the authors of a recent JAMA viewpoint titled “Shifting to Serious Illness Communication.” We discuss the debate, how to think about definitions of ACP vs serious illness communication, what should go into high quality conversations, the evidence for and against any of this, and ultimately where we go from here. Also see the image from Alex’s forthcoming editorial in JAGS, a Venn diagram of advance care planning and serious illness communication (please go to GeriPal.org to view the image). So check out the podcast and if you are interested in diving into this debate, here are some great links to learn more:
| |||
| 25 May 2023 | Group ACP and Equity: Sarah Nouri, Hillary Lum, LJ Van Scoy | 00:48:11 | |
Our guests today present an important rejoinder to the argument that we should refocus away from advance care planning (ACP). Sarah Nouri, Hillary Lum, and LJ Van Scoy argue that diverse communities are asking for ACP. Sarah Nouri gives an example from her work in the LGBTQ+ community of a trans woman who was buried as a man because existing laws/rules did not protect her wishes. Others cited the call from communities to meet them where they are - be they senior centers, Black-owned businesses, or churches (we have a podcast planned in the fall with Fayron Epps and Karen Moss on the church setting). It does seem that if communities, particularly historically marginalized communities, are interested in ACP, that fact should carry some weight in how resources are allocated to research and health care financing. We additionally have a debate/discussion about which outcomes of ACP matter most, including Terri Fried’s commentary in JAGS that caregiver outcomes matter more than goal concordant care (the “holy grail”), completion of advance directives, or changes in health care services use. Did the caregiver feel heard and understood? Did they have PTSD? Complicated grief? Depression? Group visits are one way of reaching diverse communities to which advance care planning has not traditionally been targeted. In a group visit there is a social norming effect - “if my neighbor is doing it, perhaps I should be doing it to?” Please tune in to hear more, and listen to the whistle of the “Friendship train!” -@AlexSmithMD
Links: Community Based Participatory Research and ACP in Latinx communities: https://agsjournals.onlinelibrary.wiley.com/doi/abs/10.1111/jgs.18236 Community based ACP in the Black Community: https://link.springer.com/article/10.1007/s11606-023-08134-2 ACP in the Chinese American Community: https://www.sciencedirect.com/science/article/pii/S0885392423000982 Group ACP in primary care: https://www.annfammed.org/content/14/2/125.short and https://agsjournals.onlinelibrary.wiley.com/doi/abs/10.1111/jgs.16694 Project Talk Website: www.ProjectTalkTrial.org Project Talk Trial Protocol Paper: https://journals.sagepub.com/doi/pdf/10.1177/1049909116656353 Hello Article (including Black churches): https://jamanetwork.com/journals/jamanetworkopen/article-abstract/2765685 Communication Quality Analysis: https://www.tandfonline.com/doi/abs/10.1080/19312458.2022.2099819 Conceptualizing Surrogate Decision Making: https://www.tandfonline.com/doi/abs/10.1080/19312458.2022.2099819 What counts as a surrogate decision: https://journals.sagepub.com/doi/abs/10.1177/10499091231168976
For e-training modules on ACP group visits: https://cuelearning.org Click on the Register link (upper right corner). A pop-up box will appear and enter your email address and set up your password. For Registration Code, enter: ENACT (not case sensitive). The ACP Group visit implementation guide is available here: www.coloradocareplanning.org. Scroll down to “Innovations in ACP page” | |||
| 13 Jul 2023 | Jumpstarting Goals of Care Convos: Erin Kross, Bob Lee, and Ruth Engelberg | 00:47:41 | |
Today’s podcast is a follow up to our 2018 podcast with Randy Curtis about the Jumpstart intervention. On that podcast he and collaborators tested a combined patient and clinician facing communication priming intervention to promote goals of care conversations. Today we discuss a new paper in JAMA that tests a stripped down version of the clinician only facing intervention in a pragmatic randomized trial for older adults with serious illness and those 80+. They found a difference of 4% in documented goals of care discussions. Is 4% meaningful? You’ll have to decide for yourself, though it likely is meaningful on a population basis. Intriguingly, in a sub-analysis, they found a much higher rate of difference among minoritized older adults - more like 10%. In a compelling editorial, Doug White and Sarah Anderson argue that even a 4% difference is important on a population basis, and that higher rates of difference among minoritized older adults demonstrate the potential of the intervention to address long-standing disparities in goals of care. Randy Curtis was first author of the JAMA paper. Randy died February 26, 2023. We begin today’s podcast asking his co-authors Erin Kross, Bob Lee, and Ruth Engelberg, all from the University of Washington and the Cambia Palliative Care Center of Excellence, to reflect on Randy and his dedication to seeing this work completed while living with ALS. Eric and I also reflect on the podcast Randy generously did with us on his experience living with and studying serious illness. We have lost a giant. He is sorely missed, and celebrated. And…the guests torture me about songs I can’t play with the word Jump. -@AlexSmithMD
| |||
| 20 Jun 2024 | Urinary Incontinence Revisited: George Kuchel & Alison Huang | 00:45:06 | |
I have to start with the song. On our last podcast about urinary incontinence the song request was, “Let it go.” This time around several suggestions were raised. Eric suggested, “Even Flow,” by Pearl Jam. Someone else suggested, “Under Pressure,” but we’ve done it already. We settled on, “Oops…I did it again,” by Britney Spears. In some ways the song title captures part of the issue with urinary incontinence. If only we lived in a world in which much of urinary incontinence was viewed as a natural part of aging, the normal response wasn’t embarrassment and shame, but rather an ordinary, “Oops…I did it again.” And if only we lived in a world in which this issue, which affects half of older women and a third of older men, received the research and attention it deserves. We shouldn’t have therapeutic nihilism about those who seek treatment, yet urinary incontinence is woefully understudied relative to its frequency and impact, and as we talk about on the podcast, basic questions about urinary incontinence have yet to be addressed. I don’t see those perspectives as incompatible. Today we talk with George Kuchel and Alison Huang about:
Enjoy!
| |||
| 16 Jul 2024 | Ageism and Elections: Louise Aronson and Ken Covinsky | 00:47:39 | |
Emergency podcast! We’ve been asked by many people, mostly junior/mid career faculty, to quickly record a podcast on ageism and the elections. People are feeling conflicted. On the one hand, they have concerns about cognitive fitness of candidates for office. On the other hand, they worry about ageism. There’s something happening here, and what it is ain’t exactly clear. We need clear eyed thinking about this issue. In today’s podcast, Louise Aronson, author of Elderhood, validates that this conflict between being concerned about both fitness for the job and alarmed about ageism is exactly the right place to be. We both cannot ignore that with advancing age the prevalence of cognitive impairment, frailty, and disability increase. At the same time, we can and should be alarmed at the rise in ageist language that equates aging with infirmity, and images of politicians racing walkers or a walker with the presidential seal. Ken Covinsky reminds us that we should not be making a diagnosis based on what we see on TV, and that if a patient’s daughter expressed a concern that their parent “wasn’t right,” we would conduct an in depth evaluation that might last an hour. Eric Widera reminds us of the history of the Goldwater Act created by the American Psychological Association in the 1960s which states that psychiatrists should refrain from diagnosing public figures, and the American Medical Association code of ethics which likewise discourages armchair diagnosis (rule established in 2017). We frame today’s discussion around questions our listeners proposed in response to our Tweets, and are grateful for questions from Anand Iyer, Sandra Shi, Mike Wasserman, Ariela Orkaby, Karen Knops, Jeanette Leardi, Sarah McKiddy, Cecilia Poon, Colleen Christmas, and Kai Smith. We talk about positive aspects of aging, cognitive screening, the line between legitimate concerns and ageism, ableism, advice for a geriatrician asked to comment on TV, frailty and physical disability, images in the press, historical situations including , and an upper age limit for the Presidency, among other issues. Of note, we talk about candidates from all parties today. We acknowledge concerns and speculation that others have raised about candidates across the political spectrum, current and former. We do not endorse or disclose our personal attitudes toward any particular candidate. Fitness for public office is a non-partisan issue that applies to all candidates for office, regardless of political party. There’s something happening here, and what it is ain’t exactly clear. Strong recommendation to also listen to this terrific podcast with another geriatrician all star, Jim Pacala, on MPR!
| |||
| 22 Oct 2020 | State of Heart Failure & Palliative Care: Podcast with Haider Warraich | 00:48:15 | |
There are a lot of large numbers that involve heart failure, starting with the sheer number of patients diagnosed (6.5 million and counting), to the cost of their care (~$70 billion by 2030), to the amount of money invested by the NIH into research ($1 billion annually). But the smaller numbers deserve attention too - 50% of patients die within 5 years of their diagnosis, those older than 65 in the hospital die even sooner at ~2.1 years thereafter, the median survival on hospice since hospital discharge is 11 days, and <10% of patients with heart failure receive a palliative care consult. So what can we do to bridge the gap between heart failure and palliative care? As a current palliative care fellow and former hospitalist on UCSF's Advanced Heart Failure service, I have a strong interest in this question. This week I was lucky to have Alex and Eric let me join in interviewing Haider Warraich, Associate Director of Heart Failure at the Boston Veterans Affairs Hospital and Associate Professor at Brigham and Women's Hospital, a cardiologist trained in advanced heart failure and with a strong interest in palliative care who has written multiple books (Modern Death: How Medicine Changed the End of Life, State of the Heart: Exploring the History, Science, and Future of Cardiac Disease), op eds, and research articles on the subject. In the podcast we talk about all things heart failure - from the culture of cardiology, how to impart palliative care on trainees, and practical tips on helping predict prognosis and symptom management. For more reading be sure to check out Haider's article in JPM on Top 10 Tips for Palliative Care Clinicians Caring for Heart Failure Patients and his article with Diane Meier in NEJM on Serious Illness 2.0 - Meeting the Needs of Patients with Heart Failure. - Anne Rohlfing | |||
| 29 Oct 2020 | Palliative Care for non-cancer illness: Podcast with Kieran Quinn and Krista Harrison | 00:48:51 | |
In this week's podcast we talk with Kieran Quinn, author of a systematic review and meta-analysis of palliative care for non-cancer illness, published in JAMA. We also talk with Krista Harrison, first author of an accompanying editorial. JAMA editors cut out some of my favorite parts of Krista's editorial, possibly because they were more like a blog post than a JAMA editorial. (I was senior author; go figure how it ended up reading like a blog post!) So here is the submitted introduction, unedited: "As with many people’s best ideas, inspiration struck in the shower. Dr. Balfour Mount, a urologic-cancer surgeon at the Royal Victoria Hospital in Quebec, Canada, needed a name to differentiate a new hospital-based service he created for people with serious life-threatening illness from Dr. Cicely Saunders’ English hospice programs. Dr. Mount coined the term “palliative care” to connote the core goals of the service: to improve quality of life and to mitigate sources of distress. The field of palliative care was born. The year was 1975. Forty-five years later, palliative care retains its central focus on improving quality of life for people living with serious, life-limiting illnesses and their families by addressing physical and psychological symptoms, social and spiritual needs, and aligning patient and family values with available care options." In our podcast, we talk about the surprising finding in Keiran's study that palliative care for noncancer illness was associated with a modest improvement in symptoms, reduced hospitalization and emergency department use, increased advance care planning but not improved quality of life. How can palliative care, since inception designed to improve quality of life, not improve quality of life? Listen to the podcast to find out! -@AlexSmithMD | |||
| 04 Aug 2022 | Deprescribing Super Special Part II: Podcast with Elizabeth Bayliss, Ariel Green, and Kevin McConeghy | 00:45:04 | |
A year ago we did our first “Deprescribing Super Special”. Today we are coming back for more (or less given the content), talking about the following articles with their lead authors: First up, we talk with Ariel Green about her article in JAMA Network on preferred phrases a clinician may use to explain why they should reduce or stop the medication. My take home from this is that while the most preferred explanation for deprescribing statins and sedative-hypnotics is one focused on the risk of side effects, we also need to individualize it to the patient and the medication that they are taking. Next up, we chat with Liz Bayliss about her JAMA IM article that studied whether increasing awareness about deprescribing prior to primary care visits can reduce the use of potentially inappropriate long-term medications for individuals with cognitive impairment. While the study was largely negative, it does bring up important implications about how we should think about deprescribing in older adults (added bonus too - all of the resources used in the study can be found on the US Deprescribing Research Network website). Lastly, we talk with Kevin McConeghy about one deprescribing intervention that was hugely successful, although somewhat atypical. Kevin’s study looks at a period of time in the COVID pandemic when a large multistate nursing home provider created a “nonessential medication on hold” (NEMOH) policy in order to conserve critical nursing resources and PPE, and to limit exposure risk for residents by reducing unnecessary contact. Although the policy was not originally envisioned as a deprescribing intervention, 54% of held medications were discontinued. That’s huge! While it’s unlikely this will be repeated, we talk about lessons we can learn from this natural experiment.
| |||
| 15 Oct 2020 | The Geriatric 5M Approach to Telemedicine Assessment: A Podcast with Lauren Moo | 00:39:01 | |
On todays podcast, we have Lauren Moo, a cognitive behavioral neurologist who has been doing video visits well before the COVID-19 pandemic to decrease the need for travel and to decrease the agitation in older adults with dementia that commonly occur when a clinic visits disrupts the usual routine. Now with COVID among us, Lauren talks to us about her recently published JAGS article titled Home Video Visits: 2‐D View of the Geriatric 5‐Ms. In the article and on the podcast, Lauren walks us through assessing the Geriatric 5M framework: mind, mobility, medications, multicomplexity, and what matters most. Lauren gets very practical with us about how she does things like a cognitive assessments in this new medium of telemedicine. One thing I'd like to note that we didn't talk about in our podcast, but Joe Ouslander wrote in the accompanying editors note to Lauren's article: "I recommend that you discourage patients and families from using the backgrounds of outer space, peaceful woods and lakes, or other fancy pictures that are available on Zoom, Webex, and other virtual meetings. Doing so will hide what could be extremely valuable information when assessing the M’s of geriatrics." So take a listen and maybe even sing along to Alex's version of "Video Killed the Radio Star." | |||
| 16 Sep 2021 | Living with and studying serious illness: Podcast with Randy Curtis | 00:42:52 | |
Randy Curtis, a paragon of palliative care research, was diagnosed with ALS in March. Randy is in a unique position as someone who studies and cares for people living with serious illness, who now shares his reflections on being on the other side, to reflect on the process of living with serious illness. His reflections are illuminating and inspiring. We talk with Randy about his experience being in the patient role, rather than the physician or researcher role. We ask if knowing the prognosis for his subtype of ALS is helpful to him, and if he’s seeing a palliative care clinician. We talk with Randy about his legacy, principally his focus on mentoring. We talk about how his approach to his life, his clinical work, and research has shifted in the face of living with serious illness. We end by talking about our favorite “Randy Curtis” studies. Thank you Randy for modeling vulnerability and willingness to talk about ALS. Thank you for your mentoring which has nurtured a veritable forest of trainees, and for your research which has improved care for people living with serious illness and their families. And here’s to your song choice: a “good life” indeed, by any measure. Links: -ICU family meetings: Increased proportion of family speech is associated with increased satisfaction -Alterations in translated ICU family meetings -A communication strategy and brochure for ICU family meetings -Practical guidance for ICU family meetings -Empathy in life support decisions -Cambia Center of Excellence for Palliative Care Research -Cambia Sojourns Scholars Leadership Program
-@AlexSmithMD | |||
| 03 Apr 2025 | GeriPal Takeover! Nancy Lundebjerg and Annie Medina-Walpole | 00:51:34 | |
Whelp, goodbye folks! Eric and I have been DOGE’d. In a somewhat delayed April Fools, Nancy Lundebjerg and Annie Medina-Walpole have taken over podcast host duties this week. Their purpose is to interview me, Eric, and Ken Covinsky about your final AGS literature review plenary session taking place at the Annual Meeting in Chicago this May (for those attending, our session is the plenary the morning of May 10). We discuss our favorite articles, parody songs, and memories from AGS meetings past, with a little preview of a song for this year’s meeting. We covered:
| |||
| 21 Mar 2024 | Electronic Frailty Indexes: Kate Callahan, Ariela Orkaby, & Dae Kim | 00:44:21 | |
What is frailty? Kate Callahan relates a clear metaphor on today’s podcast. A frail person is like an origami boat: fine in still water, but can’t withstand a breeze, or waves. Fundamentally, frailty is about vulnerability to stress. In 2021 we talked with Linda Fried about phenotypic frailty. Today we talk with Kate Callahan, Ariela Orkaby, & Dae Kim about deficit accumulation frailty. What is the difference, you ask? George Kushel probably explained it best in graphical terms (in JAGS), using the iconic golden gate bridge as a metaphor (Eric and I get to see the bridge daily driving or biking in to work). Phoenotypic frailty is like the main orange towers and thick orange support cables that run between towers. Damage to those critical functions and the bridge can collapse. Deficit accumulation frailty is like the hundreds of smaller vertical cables that connect the thick orange support cables to the bridge itself. Miss a few and you might be OK. But miss a bunch and things fall apart. Resilience is the ability of the bridge to withstand stress, like bridge traffic, wind, waves, and the occasional earthquake (hey it’s California!). Frailty research has come a long way. We’re now at a point where frailty can be measured automatically, or electronically, as we put in the title. Kate created an eFrailty tool that measures frailty based on the electronic health record (EHR) data. Ariela created a VA frailty index based on the EHR of veterans. And Dae created an index using Medicare Claims. Today we’re beginning to discuss not just how to measure, but how to use these electronic frailty indexes to improve care of patients. We should not get too hung up on battles over frailty. As Kate writes in her JAGS editorial, “If geriatricians wage internecine battles over how to measure frailty, we risk squandering the opportunity to elevate frailty to the level of a vital sign. Learning from the past, a lack of consensus on metrics impeded the mainstream adoption of valuable functional assessments, including gait speed.” To that end, modeled after ePrognosis, Dae and Ariela have launched a new tool for clinicians that includes multiple frailty measures, with guidance on how to use them and in what settings. It’s called eFrailty, check it out now! Did I cheat and play the guitar part for Sting’s Fragile at ⅔ speed then speed it up? Maybe…but hey, I still only have 2 usable fingers on my left hand, give me a break! -@AlexSmithMD
Additional Links: eFrailty website is: efrailty.hsl.harvard.edu (efrailty.org is fine).
The Medicare claims-based frailty index program for research: https://dataverse.harvard.edu/dataverse/cfi/
ICD-10 version Link to the code for investigators (included in the appendix): As an FYI for those in VA the code is readily available through the Centralized Interactive Phenomics Resource (CIPHER) Recent validation against clinical measures of frailty:
https://doi.org/10.1111/jgs.17027 & https://doi.org/10.1001/jamanetworkopen.2023.41915 on eFI and surgery https://doi.org/10.1111/jgs.17510 editorial in JAGS
| |||
| 12 Dec 2024 | AI for Surrogate Decision Making?!? Dave Wendler, Jenny Blumenthal-Barby, Teva Brender | 00:47:52 | |
Surrogate decision making has some issues. Surrogates often either don’t know what patients would want, or think they know but are wrong, or make choices that align with their own preferences rather than the patients. After making decisions, many surrogates experience regret, PTSD, and depressive symptoms. Can we do better? Or, to phrase the question for 2024, “Can AI do better?” Follow that path and you arrive at a potentially terrifying scenario: using AI for surrogate decision making. What?!? When Teva Brender and Brian Block first approached me about writing a thought piece about this idea, my initial response was, “Hell no.” You may be thinking the same. But…stay with us here…might AI help to address some of the major issues present in surrogate decision making? Or does it raise more issues than it solves? Today we talk with Teva, Dave Wendler, and Jenny Blumenthal-Barby about:
I’ll end this intro with a quote from Deb Grady in an editor’s commentary to our thought piece in JAMA Internal Medicine about this topic: “Voice technology that creates a searchable database of patients’ every encounter with a health care professional? Using data from wearable devices, internet searches, and purchasing history? Algorithms using millions of direct observations of a person’s behavior to provide an authentic portrait of the way a person lived? Yikes! The authors discuss the practical, ethical, and accuracy issues related to this scenario. We published this Viewpoint because it is very interesting, somewhat scary, and probably inevitable.”
| |||
| 02 Dec 2022 | Transforming the Culture of Dementia Care: Podcast with Anne Basting, Ab Desai, Susan McFadden, and Judy Long | 00:52:46 | |
What would it take to transform dementia care? While a lot of hope and money is being put into new monoclonal amyloid antibodies like lecanemab, the evidence is that while they are great in reducing amyloid in the brain for those with early Alzheimer’s disease, the effects are at best modest in slowing down the decline in cognition and function (more to be said on that in an upcoming podcast). In order to truly transform dementia care we need to think much broader than the amyloid hypothesis. So on today's podcast we invite four brilliant individuals to talk about their perspective on how to change how we as a society and health care system partner with individuals with dementia. These amazing guests include:
We discuss the importance of viewing individuals with dementia from a lens of resilience, the importance of creative engagement (as noted in Anne and Susan’s wonderful article on this subject), the role of collaborative care, and what we can do to improve inclusivity for individuals with dementia in our community and health care systems.
| |||
| 17 Jun 2021 | Neighborhood-Disadvantage and Health: A Podcast with Amy Kind | 00:42:48 | |
What if there was a tool that could break down a neighborhood’s socioeconomic measures, like income, education, employment and housing quality, to give us a sense of how those factors influence overall health, and maybe even inform where to target health resources and social interventions. On today’s podcast we talk with Dr. Amy Kind from the University of Wisconsin School of Medicine and Public Health, who developed that tool, the Neighborhood Atlas. The Neighborhood Atlas uses the “Area Deprivation Index,” which includes 17 measures of education, housing quality and poverty, and can be used free by anyone by going to the Neighborhood Atlas website (https://www.neighborhoodatlas.medicine.wisc.edu/). In addition to talking with Amy about the Atlas, we discuss some of the following questions:
So take a listen and if you want to read more about it, check out Amy’s NEJM article on the topic - https://www.nejm.org/doi/full/10.1056/NEJMp1802313 | |||
| 18 Nov 2021 | Every deep drawn breath: Podcast with Wes Ely | 00:52:57 | |
Though “breath” is in the title of Wes Ely’s book (and his song choice by the Police), relationships are its beating heart. The book operates on two levels. On one level, Wes Ely’s book is an autobiography of a critical care doctor’s horror and shame at discovering that his ICU practice of heavily sedating patients for days on end was leading to lifelong physical, cognitive, and psychological harm; and the arc of his redemptive journey to find a better way to care for patients in the ICU. But this book also operates on a second, much deeper level. On this deeper level the book is a story of Wes Ely’s journey toward rediscovering the humanity in medicine by forging deep, lasting connections with his patients. We begin and end today’s podcast at this deeper level, talking about the spiritual connections, that doctors can forge caring for critically ill patients. (quick plug: next week’s podcast is with Chaplains on Spirituality and Palliative Care). We are joined today by Lekshmi Santhosh, head of UCSF’s post-COVID and post-ICU clinic, to interview Wes about these themes that animate his book, and more, including how we lost our way in treating ICU patients during COVID, returning to the practice of heavily sedating patients for days on end. Of note, Wes is donating proceeds from his book to the CIBS center, to benefit research and patient care to improve care for people with critical illness, during and after the ICU stay.
| |||
| 02 Jun 2022 | What We Now Know About COVID Prevention and Treatment: A Podcast with Monica Gandhi | 00:51:32 | |
We are two and a half years into the COVID pandemic. We’ve lived through lockdowns, toilet paper shortages, mask mandates, hospital surges where ICU’s overflowed, a million COVID deaths, prolonged school closures, development and roll out of novel vaccines, an explosion of social isolation and loneliness, and the invention of the “zoom meeting.” But what have we really learned over this seemingly endless pandemic other than how to make a quarantini? Well, on today’s podcast we invite Monica Gandhi to sum up the evidence to date about how best to prevent getting COVID (or at least the severe outcomes of the disease) and how to treat it, including the role of Paxlovid in symptomatic disease. Monica Gandhi is a professor of medicine and associate division chief of HIV, Infectious Diseases, and Global Medicine at UCSF & San Francisco General Hospital. In addition to her research publications, she is a prolific writer both on social media and on media outlets like the Atlantic and the Washington Post. Some call her an optimist or maybe a pragmatist, but I’d call her someone who inherently understands the value in harm reduction when it’s clear harm elimination just ain’t gonna happen. So take a listen and if you want a deeper dive into some of the references we discuss on the podcast, here is a list:
| |||
| 15 Aug 2024 | Anti-Asian Hate: Russell Jeung, Lingsheng Li, & Jessica Eng | 00:46:00 | |
Anti-Asian hate incidents rose dramatically during COVID, likely fueled by prominent statements about the “Chinese virus.” VIewed through the wider lens of history, this was just the latest in a long experience of Anti-Asian hate, including the murder of Vincent Chin, the Chinese Exclusion Act, and the internment of Japanese Americans during WWII. For those who think that anti-Asian hate has receded as the COVID has “ended,” just two days prior to recording this episode a Filipino woman was pushed to her death on BART in San Francisco. These incidents are broadcast widely, particularly in Asian News outlets. Today we talk about the impact of anti-Asian hate on the health and well being of older adults with Russell Jeung, sociologist, Professor of Asian Studies at San Francisco State, and co-founder of Stop AAPI-Hate, Lingsheng Li, geriatrician/palliative care doc and T32 fellow at UCSF, and Jessica Eng, medical director of On Lok, a PACE, and Associate Professor in the UCSF Division of Geriatrics. We discuss:
See also guides for how to confront and discuss anti-Asian hate in these articles in the NEJM and JGIM. And to balance the somber subject, Lingsheng requested the BTS song Dynamite, which was the group’s first English language song, and was released at the height of the COVID pandemic. I had fun trying to make a danceable version with electronic drums for the audio-only podcast. Maybe we’ll get some BTS followers to subscribe to GeriPal?!?
-@AlexSmithMD
| |||
| 05 Oct 2023 | The Language of Serious Illness: A Podcast with Sunita Puri, Bob Arnold, and Jacqueline Kruser | 00:46:12 | |
Communicating about a serious illness is hard. Last week’s podcast we talked about the challenge around miscommunication in serious illness. This week we dive into the challenges with communication when it comes to life sustaining treatments and CPR. Take for example the simple question:
We’ve invited Jacqueline Kruser and Bob Arnold on this week's podcast to talk about their recently published JAMA Viewpoint article titled “Reconsidering the Language of Serious Illness.” I love this article as it specifically discusses what’s wrong with “need” statements and how we can shift our communication and thinking to create space for deliberation about patients’ priorities and the best course of action. We’ve also invited Sunita Puri to talk about the language of life sustaining treatments, in particular CPR. Sunita recently published a wonderful New Yorker article titled The Hidden Harms of CPR arguing among other things that these conversations “are procedures, demanding the same precision of everything else in medicine.” So take a listen and check out some of these other links to dive deeper:
| |||
| 29 Feb 2024 | GeriPal 300th Episode: Ask Me Anything Hot Ones Style | 00:43:48 | |
Today we celebrate eight years, around 2 million listens, and 300 podcasts!
Eric and I take questions from you, our listeners, about: why we podcast, our most controversial podcast, which podcast changed our practice, favorite song request, should all nursing home residents complete the POLST, expanding access to durable medical equipment, palliative care in rural regions, do we have an advance directive, what we’d do to improve healthcare with 7 trillion dollars, treatment for poor appetite, and Eric on how to make a latte. Thank you to Lynn Flint and Anne Kelly who serve as hosts for this episode, asking us the tough questions. We answer your questions hot ones style. I borrowed some screaming hot sauces from my friends Jerome Kim and Tony Le, and added them to my small collection of extra mild sauces. Every two questions we ate a chicken wing covered in hot sauce. The hot sauces progressed from mild to extreme (and I mean extreme) heat. Can I just say…it works? Being asked a question with your mouth on fire, sweat streaming down your face, feeling the most awake and terrified you have ever been in your life, forces you to give an unadorned answer, straight from the heart. Don’t take my word for it, listen for yourself! Or better yet, watch the video of this one on YouTube. Some of the funniest parts are caught on video, in the background. We will be re-watching this one for years to come. Thank you, dear listeners, for sending us your questions, for your enthusiasm, and for your support. Enjoy! -@AlexSmithMD
| |||
| 15 Feb 2024 | EMS Intervention to Reduce Falls: Carmen Quatman and Katie Quatman-Yates | 00:45:33 | |
We've talked about Falls a couple of times on this podcast, most recently with Tom Gill about the STRIDE study and before that with Sarah Szanton about the CAPABLE study. A takeaway from those podcasts is that fresh innovative thinking in the falls prevention space is welcome. Today we talk with the twin sister power duo of Carmen Quatman and Katie Quatman-Yates about an intervention that is both brilliant and (in retrospect) should have been obvious. The insight started when Carmen, an orthopedic surgeon-researcher, and Katie, a physical therapist- researcher participated in ride-alongs with EMS providers to patient’s homes. They were stunned by the number of calls for lift assistance for older adults who had fallen. Going into patient's homes was eye opening. There were trip hazards, loose carpets, some people were hoarders. And yet, after assisting the older adult to their feet, the EMS providers would leave. Their job was done. It's not surprising that the number of repeat calls for falls is alarmingly high. Addressing the root environmental causes of falls was not part of EMS providers' job description. In addition to stigma, practical barriers to older adults addressing environmental issues themselves abound. For example, Carmen and Katie found thousands of grab bars on Amazon (overwhelming), and when they called installation companies (handypersons), received different quotes if the person calling was a man or a woman. So Carmen and Katie developed an EMS Community Partnership program. EMS providers were trained to provide practical home modifications: installation of grab bars, removal of carpets, removal of other obstacles. They created a seamless link between this Community Partnership program and 911 calls for falls. People who had grab bars installed through the program called their neighbors and say, hey you should get this too. Word of mouth spread rapidly. And the number of calls for falls dropped. Eric and I enjoyed talking with Carmen and Katie about this innovative and common sense approach to addressing falls in the community. In addition to the podcast, you can see more about this in Carmen's TEDx talk. Thanks to my wife Cindy Hsu for piano on Eye of the Tiger. Enjoy! -@alexsmithMD
| |||
| 30 Jan 2025 | Telehealth vs In-Person Palliative Care: Guests Joseph Greer, Lynn Flint, Simone Rinaldi, and Vicki Jackson | 00:51:14 | |
It is a battle royale on this week’s GeriPal podcast. In one corner, weighing in at decades of experience, well known for heavy hits of bedside assessments, strong patient-family relationships, and a knockout punch of interdisciplinary collaboration, we have in-person palliative care consults. But watch out! Travel time can leave this champ vulnerable to fatigue and no-shows. In the other corner, we have the young upstart, able to reach patients across vast distances when delivering palliative care, all in the comfort of wearing pajamas, we have telehealth delivered palliative care. However, lack of physical presence may make this contender struggle to land the emotional support punch that is at the very heart of palliative care. Who will emerge victorious? Will in-person palliative care use its experience and bedside manner to overwhelm telehealth palliative care, or will telehealth deliver the knockout blow of efficiency and accessibility? Find out on this week’s podcast where we invite Joseph Greer, Simone Rinaldi, and Vicki Jackson to talk about their recent JAMA article on “Telehealth vs In-Person Early Palliative Care for Patients With Advanced Lung Cancer - A Multisite Randomized Clinical Trial.” Additionally, here are some of the resources we talked about during the podcast:
| |||
| 20 Feb 2025 | Trauma-Informed Care: A Podcast with Mariah Robertson, Kate Duchowny, and Ashwin Kotwal | 00:47:07 | |
Trauma is a universal experience, and our approach as health care providers to trauma should be universal as well. That’s my main take-home point after learning from our three guests today when talking about trauma-informed care, an approach that highlights key principles including safety, trustworthiness, peer support, collaboration, empowerment, and cultural sensitivity. With that said, there is so much more that I learned from our guests for this trauma-informed care podcast. Our guests include Mariah Robertson, Kate Duchowny, and Ashwin Kotwal. Mariah discussed her JAGS paper on applying a trauma-informed approach to home visits. Kate and Ashwin talked about their research on the prevalence of lifetime trauma and its association with physical and psychosocial health among adults at the end of life. We also explored several questions with them, including how to define trauma, its prevalence in older adults, the impact of past traumatic experiences, the potential triggers of trauma screening, and the application of trauma-informed principles in clinical practice. If you want a deeper dive, check out the following resources:
| |||
| 20 Jan 2022 | Medicare Advantage, Special Needs Plans, and the Hospice Carve-In: A podcast with Dr. Claire Ankuda and Dr. Cheryl Phillips | 00:45:35 | |
More Health Policy this week! Today, we discuss “SNPs” but this is not a podcast about haircuts during the pandemic. We take a deeper dive into the world of Medicare Advantage and what it means for vulnerable patients facing serious illness and those at the end of life. We are joined by UCSF geriatrics fellow Alex Kazberouk to talk to Dr. Claire Ankuda (Assistant Professor at Icahn School of Medicine at Mount Sinai and Palliative Care Physician) and Dr. Cheryl Phillips (President and CEO of the Special Needs Plan Alliance and past president of the American Geriatrics Society). We discuss:
This is part two of a two part series on Medicare Advantage and healthcare financing. On our prior episode, we heard Dr. Don Berwick’s and Dr. Rick Gilfillan’s critique of Medicare Advantage plans. This week, we bring up a rebuttal to their critique and also talk about quality data and reporting for Medicare Advantage patients. Alex plays The Purchaser’s Option by Rihannon Giddens (she has so many terrific songs!). Astute online viewers will also spot an appearance of the Team Canada Tokyo 2021 Olympic Jacket and Cheryl’s dog. | |||
| 08 Sep 2022 | Prolonged Grief Disorder: Holly Prigerson | 00:46:14 | |
Holly Prigerson recalls the moments in which she started investigating prolonged grief disorder. She recalls being “a social scientist [Holly] in room a full of psychiatrists,” who recognized a diagnostic gap in people experiencing profound and potentially harmful grief far after the death of a loved one. This led her on a remarkable journey. Holly has accumulated mountains of evidence for the diagnosis of prolonged grief disorder as a specific condition primarily notable for a yearning over a year after the death. Prolonged grief is associated with increased risk of suicide and other negative health outcomes. This accumulation of data over her career led ultimately to the inclusion of Prolonged Grief Disorder first in the ICD, then in the DSM-V. And yet, despite mountains of evidence, Holly has taken a tremendous amount of heat for this work. “Everyone has experienced grief, which makes everyone the expert.” Today we offer Holly a chance to answer her critics, including assertions that:
Along the way we talk about other related studies Holly has conducted, including a validation of DABDA - Elizabeth Kubler Ross’s famous stages of grief. And a song choice from the great lyricist Tom Waits. Enjoy! -@AlexSmithMD | |||
| 17 Apr 2025 | Loss of DEI Hurts Everyone: Farah Stockman, Ali Thomas, Ken Covinsky | 00:47:18 | |
I read Farah Stockman’s article in the NYT on why attacks on DEI will cost us all, and thought, “Yes, and ‘everyone’ includes harm to our healthcare workforce, our patients, and their families.” So we’re delighted that Farah Stockman, pulitzer prize winning journalist, author of American Made: What Happens to People When Work Disappears, and editorial board member at the New York TImes joins us to set the bigger picture for this discussion. Farah provides clear examples from the Biden administration, in which having the most diverse cabinet in history was critical to building bridges, empathy, and inspiring others to feel included. We are also pleased to welcome Ali Thomas, a hospitalist, member of the Baha'i Faith, leader of anti-racism efforts in the Pacific Northwest, and founder of the BIPOC Health Careers Ecosystem. Ali talks about the history of affirmative action, which started as a program for Whites, the importance of diversity in the healthcare workforce, the history of allyship and cross cultural collaboration, and his own efforts to provide opportunity and support for historically oppressed groups in his own community to obtain healthcare careers. And Ken Covinsky, avid baseball fanatic, joins us and notes that the day we record (April 15) is Jackie Robinson day. Many may be familiar with the story of Jackie Robinson breaking the color barrier in major league baseball in 1947, but may not be aware of the tremendous adversity Jackie Robinson faced, and persistence he displayed, off the field. We address many things, including:
There was so much we hoped to talk about and didn’t get to, but I will link to now, including: Ali’s mom’s personal history with and study of school desegregation in South Carolina, Farah’s mom’s pioneering work as a speech language pathologist, and Ken’s perspectives on the importance of studying ageism and racism in research. What a Wonderful World could be sung in irony at this moment. I hope we all take it literally, with the hope this podcast ends with. -Alex Smith
| |||
| 14 Oct 2021 | Primary Palliative Care for Cancer: Podcast with Yael Schenker and Bob Arnold | 00:46:51 | |
“The take home message of this study is NOT that primary palliative care does not work.” So says Yael Schenker of the negative study of an oncology nurse-led primary palliative care intervention for people with advanced cancer. And we pushed Yael and Bob Arnold (senior author) on this point - we have several negative studies of primary palliative care (see links below to podcasts) - is it time to start to question the effectiveness of primary palliative care? We certainly all agree on the problem: we have only enough palliative care specialists to care for some small proportion of the population of people with serious illness. But when we move away from specialist palliative care to primary palliative care do we lose something critical? Perhaps we cannot train primary providers (front line nurses and doctors generally) to deliver palliative care that is “good enough” to impact outcomes. That’s one interpretation. Another is that we need a “stronger dose” of primary palliative care. In Yael and Bob’s study nurses averaged 2.2 visits, hardly robust longitudinal palliative care. Patients who had 3 visits had better outcomes. Unpacking negative studies is just as interesting as unpacking positive studies. Knowing what doesn’t work is just as important as knowing what does. Links:
| |||
| 27 Jan 2022 | End Stage Liver Disease: Podcast with Jen Lai, Ricky Shinall, Nneka Ufere, and Arpan Patel | 00:51:21 | |
Patients with end stage liver disease and decompensated cirrhosis have an average life expectancy of 2 years without transplant. Outcomes are worse among those who are frail. Symptoms are common, including pain, ascites, encephalopathy, and pruritus. Patients with end stage liver disease are often some of the most disadvantaged patients we care for. Caregiver burden is immense; divorce is common. Some will go on to receive a transplant, but many will not. Many are confused about the diagnosis and feel poorly supported. Prognosis is fraught, as the worse your prognosis (i.e. lower your chance of survival), the higher you move on the transplant list. Advance care planning is rare (or serious illness communication for those of you who don’t consider this advance care planning). Outcomes of in-hospital CPR are worse for patients with end stage liver disease than outcomes for patients with advanced cancer. Though integration of geriatrics and palliative care into the care of patients with end stage liver disease holds obvious potential, major barriers remain. In this week’s podcast, we talk with Jen Lai, Ricky Shinall, Nneka Ufere, and Arpan Patel about end stage liver disease from a geriatrics and palliative care perspective. We talk about the tension patients face between putting on the “best face” to be listed for transplant (e.g. full code, goals focused on extending life). We talk about the potential and limitations of the MELD score for prognosis, and how frailty further stratified risk for older patients with end stage liver disease. We discuss what is needed in terms of improved communication around the time of diagnosis, creating a safe space for serious illness communication, and resources for patients and caregivers (including this Canadian information resource). And we have a round robin about treatment of common and challenging symptoms – yogurt makes a surprise appearance. And…Radiohead! Great request…thank you Nneka! -@AlexSmithMD | |||
| 13 Oct 2022 | Updates in ID and Nephrology: Lona Mody, Rasheeda Hall, Devika Nair, Sonali Advani | 00:48:01 | |
When I’m on service these days there is inevitably a moment when a resident says “Patient so-and-so is on X” - and I have absolutely no idea what X is. Modern subspecialist practice advances at such a remarkably rapid pace, it can be hard to keep up. In this context, we’re excited to hear from infectious disease experts and nephrologists about updates in the care of older adults. Sonali Advani and Lona Mody talk about their recent JAGS article highlighting three recent articles that every clinician caring for older adults should be aware of in the treatment of infectious diseases (hint: I’ve never finished a course of antibiotics, and maybe your patients don’t need that full course either). Devika Nair and Rasheeda Hall talk about their JAGS article highlighting updates from nephrology in the care of older adults, including a link to this new eGFR calculator that does NOT include race. We have a discussion about the decision to remove race, a social construct, from clinical risk calculators (though I’m not 100% sold that race should always be removed - if removal is likely to worsen disparities for example - at least until a superior race-blind calculator can be developed). These articles are part of a new series called Clin-Star Corner, a new series in JAGS that reviews practice changing articles in the care of older adults. And yeah, they made me sing a Miley Cyrus song…(but not this hilarious parody about UTIs). Enjoy! -@AlexSmithMD | |||
| 29 Jun 2023 | Hospice in Prison Part 2: An interview with the Pastoral Care Workers | 00:46:48 | |
I don't know 'bout religion These are the ending lyrics to Bonnie Raitt’s song “Down the Hall”, an ode to the Pastoral Care Workers who care for their fellow inmates in the hospice unit at the California Medical Facility in Vacaville, California. On last week’s podcast we interviewed the medical director and the chaplain of the prison’s hospice unit (Hospice in Prison Part 1). This week we turn our attention to the inmates. Pastoral Care Workers are inmates who volunteer time to care for the dying who come from all around California to spend their last days, weeks or months in the prison’s hospice unit, fulfilling a mission that “no prisoner dies alone.” On today's podcast we talk with three of these Pastoral Care Workers, Jerry Judson, Jeffrey Maria, and Allan Krenitzky. We discuss with them why they decided to volunteer for the hospice unit, what a day in the life of a Pastoral Care Worker looks like, and among other things their thoughts on forgiveness, redemption, rehabilitation, and compassionate release. We also had the pleasure to take a walk through the hospice unit garden with Mr. Gerald Hite. He taught us a little about the different flowers and plants, and along the way a little about why he does what he does. While this is a podcast about volunteers in a prison hospice, I think it also serves as a lesson for us all about how we make meaning to our own lives and define ourselves by not only what we have done in the past, but what we do now. One story that Allan told perfectly sums this up. He said one day his son asked his wife what he does for a living, and his wife said “Papa helps sick people.”
| |||
| 07 Oct 2021 | Time Limited Trials in the ICU: A Podcast with Dong Chang and Richard Leiter | 00:47:13 | |
Time-limited trials. We’ve all probably used them before. We meet with patients and families. We agree to either start or continue a particular treatment to see if it helps in some specific way over some defined period of time. If it works as hoped, great, we continue the treatments. If not, we stop them. At least that is how it’s supposed to go. On today’s podcast we talk all about these time-limited trials with Dong Chang and Ricky Leiter. Dong was the lead author of a JAMA IM article looking at the outcomes of training staff to use time-limited trials as the default communication and care planning approach for critically ill patients in intensive care units. Ricky is the lead author of the accompanying editorial and palliative care physician extraordinaire. We discussed with Dong and Ricky about the results of the JAMA IM study, which were pretty darn impressive. The intervention resulted in significant reductions in duration of ICU stay (7.4 v 8.7 days), fewer invasive procedures, but no change in mortality, and no change in family satisfaction rating (which was high before and after the intervention). We discuss potential reasons why the intervention worked, some limitations of the study, the role uncertainty plays in decision-making, and so much more (including nudging from our last podcast). If you want to read more about time-limited trials, check out these articles as well:
| |||
| 31 Oct 2024 | COVID Updates: A Podcast with Peter Chin-Hong and Lona Mody | 00:43:56 | |
In March 2020, we launched our first podcast on COVID-19. Over the past four years, we’ve seen many changes—some positive, some negative. While many of us are eager to move past COVID (myself included), it’s clear that COVID is here to stay. This week, we sit down with infectious disease experts Peter Chin-Hong and Lona Mody to discuss living with COVID-19. Our conversation covers:
We wrap up with a “magic wand” question. My wish was for better randomized evidence for vaccines and treatments, though I worry this might not be feasible. In the meantime, there’s significant room to improve vaccine uptake among high-risk groups, particularly nursing home residents. Currently, only 1 in 5 nursing home residents in the US have received the COVID booster, compared to over 50% in the UK. By: Eric Widera
| |||
| 03 Jun 2021 | "Palliative" Inotropes?!?: Podcast with Haider Warraich | 00:46:16 | |
In your clinical experience, you may have cared for patients receiving palliative chemotherapy and wondered, hmmm, why is that called “palliative” chemotherapy? We’ve written about this issue previously here at GeriPal (“a term that should be laid to rest”) as has Pallimed (“an oxymoron”). Well, now we have “palliative” inotropes for people with heart failure. And we have to ask, is this a fitting term? And the answer is...complex...more so than you might think. Recall that in one of our earliest podcasts, we talked with Nate Goldstein who memorably proclaimed “the best palliative care for heart failure is treatment for heart failure.” To unpack the issue of palliative inotropes, we welcome back Haider Warraich, a cardiologist with a strong interest in palliative care. We are joined again by Anne Rohlfing, palliative care fellow at UCSF who spent last year as a hospitalist on the heart failure service. Please tune in to hear more about the role of palliative care in inotrope therapy, inotropes in hospice, Haider’s study on palliative needs of patients with heart failure, and a bit about Left Ventricular Assist Devices (including a shout out to Dan Matlock’s decision aids) and Haider’s Journal of Palliative Medicine paper on top 10 tips for palliative care clinicians on caring for patients with LVADs. -@AlexSmithMD | |||
| 06 Jan 2022 | Amyotrophic lateral sclerosis (ALS) - What every Geriatrician and Palliative Care Clinician Should Know | 00:49:55 | |
Three months ago we did a podcast with Randy Curits about his recent diagnosis of ALS in March and what it was like for someone who studies and cares for people living with serious illness, to now be someone who is living with serious illness. It was one of our favorite podcasts we’ve done, but also got us to think “wait, how come we’ve never done a podcast on ALS?” We fix that on today’s podcast. We’ve invited Elizabeth Lindenberger and Kara Bischoff to talk about what every geriatrician and palliative care clinician should know about ALS. Topics include: prognosis in ALS, disease modifying therapies (and when/if to discontinue, advance care planning in ALS, the role of embedding geriatrics/palliative care in ALS clinics, interventions in ALS (noninvasive ventilation, PEG tubes, and trachs), and symptom management as the disease progress. So take a listen and if you want to take a deeper dive, take a look at these articles:
| |||
| 30 May 2024 | Palliative Care for Kidney Failure: Sam Gelfand, Kate Sciacca, and Josh Lakin | 00:45:48 | |
The landscape of options for treating people with kidney failure is shifting. It used to be that the “only” robust option in the US was dialysis. You can listen to our prior podcast with Keren Ladin talking about patients who viewed dialysis as their only option, and structural issues that led to this point (including this takedown of for profit dialysis companies by John Oliver). One of the problems was a lack of an alternative robust option to offer patients. As one of our guests says, you have to offer them something viable as an alternative to dialysis. Today we interviewed Sam Gelfand, dually trained in nephrology and palliative care, Kate Sciacca, a nurse practitioner (fellowship trained in palliative care), and Josh Lakin, palliative care doc, who together with a social worker and other team members started KidneyPal at DFCI/BWH, a palliative care consult service for people with advanced kidney disease. As a team, they provide a robust alternative to dialysis for patients with kidney failure: conservative kidney management. And “conservative,” as they note, can mean not only a “conservative approach,” as in non-invasive/less aggressive, but also an effort to “conserve” what kidney function remains. We get right down to the nitty gritty of kidney supportive care techniques they incorporate in clinic, including:
Our guests were deeply grateful to their colleagues Dr. Frank Brennan, Dr. Mark Brown, and clinical nurse consultant Elizabeth Josland of the renal supportive care team at St. George Hospital in Sydney, Australia (down under) for teaching them the ropes of palliative care in kidney failure. And we got to learn some new vocabulary, including the meaning of “chunder.” Enjoy!
| |||
| 27 May 2021 | All Things Caregivers: Podcast with Chanee Fabius and Halima Amjad | 00:41:31 | |
What is a care manager? In this week’s podcast we talk with Chanee Fabius, who after a personal experience caring for a family member with dementia, became a care manager. Chanee explains in clear terms what a care manager is, what training is required, and what training is required. In essence, a care manager is a “glue person” who hold things together. After observing major race/ethnic disparities in caregiving, Chanee was inspired to obtain a doctoral degree in gerontology, and her research is now directed toward reducing disparities in caregiving, particularly for patients with dementia. See for example, her recent paper in the Gerontologist describing Black and White differences in caregiving. We are also joined by Halima Amjad, a geriatrician-researcher, who, like Halima, is at Hopkins. Halima is very interested in improving care for people with dementia. As she notes, when we talk about outcomes for older adults, we often talk about the characteristics of the patient as predictors, but rarely do we consider how caregiver factors might influence important outcomes for older adults. In a paper published in JAGS, Halima found that caregiver factors predict hospitalization. For example, caregivers who are new to the caregiving role are more likely to care for someone who is subsequently hospitalized than someone who has been caregiving for longer. We talk about all things caregivers, including research issues around the need to assess the needs of caregivers, health policy issues such as how to provide more support for caregivers, and clinical issues, such as the fact that the identity and contact information for caregivers are not routinely captured in the EHR. -@AlexSmithMD | |||
| 29 Jul 2021 | Aducanumab (Aduhelm) for the Treatment of Alzheimers: A Podcast with Aaron Kesselheim and Jason Karlawish | 00:44:23 | |
On June 7th, 2021 FDA approved the amyloid beta-directed antibody aducanumab (Aduhelm) for the Treatment of Alzheimers. This approval of aducanumab was not without controversy. Actually, let me restate that. The approval of aducanumab was a hot mess, inside a dumpster fire, inside a train wreck. After the approval, three members of the FDA advisory panel, which unanimously was not in favor of the approval of aduhelm, quit. One of them, Aaron Kesselheim (who we have on our podcast today) described it as “the worst drug approval decision in recent U.S. history" in his resignation letter. Then the FDA had to revise the label one month after publishing it because the original didn't even come close to looking like the population in which treatment was initiated in clinical trials. Then, wait for it, after a firestorm of criticism the FDA’s commissioner had to ask for an independent investigation to look into the interactions between Biogen representatives and FDA members. And now CMS is deciding if and how to cover Aduhelm, a drug that will cost at least $56,000 a year per patient not incluiding the doctor’s visits, amyloid PET scans, and frequent MRIs that will be necessary to monitor for side effects. On today's podcast we talk all about aducanumab with Aaron Kesselheim, Professor of Medicine at Harvard Medical School and previous member of that now famous FDA advisory committee, as well as Jason Karlawish, Professor of medicine, medical ethics and health policy, and neurology at the University of Pennsylvania Perelman School of Medicine. I’d love to point you to the journal articles for the two phase III trials on aducanumab, but as of yet, they are unpublished (this should tell you a little about the faith Biogen has on its drug data), so I’ll leave you with these resources instead:
The last one is particularly important as whether you are for or against the coverage of aducanumab, your voice matters. There is a letter being circulated by physicians who care for people with Alzheimer's Disease urging CMS not to cover aducanumab given the limited clinical evidence for benefit, known harms, and exorbitant cost. You can find the letter here. If you would like to sign the letter, you can add your name by clicking this link.
| |||
| 22 Feb 2024 | Psychological Issues in Palliative Care: Elissa Kozlov and Des Azizoddin | 00:45:44 | |
In our podcast with palliative care pioneer Susan Block, she identified the psychological/psychiatric aspects of palliative care as the biggest are of need for improvement. As she said, when you think about the hardest patients you’ve cared for, in nearly all cases there was some aspect of psychological illness involved. That rings true to me. Today we talk with two psychologists who are deeply invested in addressing psychological aspects of care for people living with serious illness. Elissa Kozlov, a geropsychologist and director of a new population aging MPH at Rutgers, surveyed AAHPM members, and found that doctors reported major shortcomings in level of comfort and knowledge caring for patients with psychological illness. She conducted a systematic review and meta-analysis of 38 palliative care trials, finding that many excluded people with serious illness, and a lack of impact on psychological outcomes. Analyzing the Health and Retirement Study, she found 60% of older adults screened positive for depression in the last year of life (related study here). Des Azizoddin is a psychologist at the University of Oklahoma primarily focused on pain for people with cancer. Des delivered a plenary at this year’s National Palliative Care Research Center’s Foley retreat. She began by asking, “Raise your hand if you think there is a psychological component to cancer pain.” All hands go up. Then, “Keep your hand up if you frequently refer patients with cancer pain to a psychologist?” All hands go down. Unfortunately, we lack the financial structures to reimburse psychologists that would incentivize widespread inclusion on palliative care teams. Because we live in the world as it is, not as it should be, Des has helped develop an app (link to pilot trial hot off the press!) to help people with cancer pain engage in cognitive behavioral therapy in bite sized 3-4 minute sessions (there are other apps available now developed in the VA, who have been leaders in the psychology/palliative care space). Des additionally studied stigma associated with opioid use among patients with cancer in the context of the opioid epidemic; depression, pain catastrophizing, recent surgery and opioid use among people with cancer. And, we talk about these issues and more (with far more nuance than I can include in this post). Kudos and credit to my son Renn, age 15, for the guitar on Heartbeats (hand still broken at time of recording).
| |||
| 12 Oct 2023 | Surgical Communication: A Podcast with Gretchen Schwarze, Justin Clapp and Alexis Colley | 00:51:55 | |
For surgeons and patients, deciding if and when to operate can be challenging. Often, the way surgeons communicate about these decisions doesn’t make things any easier for themselves or their patients. And, surgeons often spend the majority of their conversations with patients describing anatomical details and exactly how they plan to ‘fix it’, with little discussion of what that ‘fix’ will do for a patient’s overall goals. Instead, what if your surgeon told you that the operation she was discussing could help with only 4 things: live longer, feel better, prevent disability, or obtain a diagnosis? And, what if your surgeon openly discussed the expected ‘bad stuff’ of post-operative recovery, instead of rotely reciting a list of possible complications? We invited Gretchen Schwarze and Justin Clapp to discuss with us these communication strategies, which are the focus of a series of 4 Viewpoints recently published in JAMA Surgery. I love this series of articles because each presents a component of a practical, patient-centered approach to patient-surgeon communication and decision making, and language surgeons (and surgical trainees) can start using in their next patient visit. We hope you enjoy this episode. Take a look at some of these links to learn more:
By: Alexis Colley
| |||
| 25 Feb 2021 | So you want to be a hospice medical director? Podcast with Tommie Farrell and Kai Romero | 00:45:22 | |
So what exactly does a hospice medical director do? Why do some choose to become hospice physicians? What additional training is needed, if any, beyond Hospice and Palliative Medicine fellowship and boards? Who should take the new Hospice Medical Director Certification Board Examination? A recent study in JAGS found high rates of hospice disenrollment (“live discharge”) for people with dementia - is that a good thing or a bad thing? Hmmm… We address these and other questions in this week’s podcast with Tommie Farrell, hospice physician in West Texas and Chair of the Hospice Medical Director Certification Board, and Kai Romero, Chief Medical Officer for Hospice By the Bay (that’s San Francisco Bay). And I get a re-do attempt at REM’s “Everybody Hurts!”. Apologies for the first attempt! -@AlexSmithMD | |||
| 28 Jul 2022 | Palliative care for cancer: Podcast with Jennifer Temel and Areej El-Jawahri | 00:51:26 | |
We are fortunate today to interview two oncologists whose research has catapulted palliative care forward: Jennifer Temel, author of the landmark NEJM study on early outpatient palliative care for patients with advanced lung cancer; and Areej El-Jawahri, author of the landmark JAMA article on inpatient palliative care for patients with blood cancers undergoing stem cell transplant. Jennifer’s study is most widely known for the “kicker” - not only did it improve quality of life, palliative care was associated with a couple months longer survival. Areej’s study is remarkably novel in that it is, to our knowledge, the first study of palliative care during curative treatment. We cover a huge amount of ground today, including:
Additional links:
| |||
| 17 Feb 2022 | Bisphosphonates for Osteoporosis: Podcast with James Deardorff and Sei Lee | 00:45:08 | |
My mom is an Asian woman in her 70s with osteoporosis. She tried an oral bisphosphonate and had horrible esophagitis. She said never again, though she eventually tried an IV bisphosphonate. She had terrible flu-like symptoms. She said never again. But based on reports that symptoms are worse the first time, she tried the IV again the next year and fortunately experienced no symptoms. (Story used with permission, thanks mom!). I tell this story because these issues don’t typically register as more than a nuisance for clinicians, who frequently don’t understand why their older patient with osteoporosis is not taking a bisphosphonate. But our patients are walking with their feet, and adherence to bisphosphonates for osteoporosis is poor and decreases with time. When we have a medication with up front harms and downstream benefits, it’s critical that we consider the time to benefit, or how long it will take an individual to benefit from a test or treatment. Think of the 10 years it takes to benefit from colon or breast cancer screening, which is designed to detect slow growing cancers. For individuals with a life expectancy less than the time to benefit, the up front harms outweigh the downstream benefits. In this context, we talked this week with James Deardorff and Sei Lee about their study of time to benefit of bisphosphonates for osteoporosis, published in JAMA IM. What they found somewhat surprised us: it’s pretty short, about 1 year! Which makes me feel better about urging my mom to get treatment. Bisphosphonates are pretty darn effective, and act quickly. We also discuss discontinuing bispohsophantes, and if we can use the same logic we consider when starting them. Toward the end we talk about the launch of ePrognosis’ new Time to Benefit tool. This tool provides a clinical recommendation for starting/stopping medications and cancer screening based on the prognosis of the patient in front of you. See screenshot below. You can either access it directly here. I you use the Lee Schonberg prognostic index for community dwelling older adults you will be directed to the tool, and it will automatically place the life expectancy at the calculated prognostic estimate. James and Sei requested a terrific song - Bad to the Bone - much better than the Hannah Montana Bone Dance song they threatened me with (maybe next time). Enjoy! -@alexSmithMD | |||
| 31 Aug 2023 | Normalcy, introspection, & the experience of serious illness: Bill Gardner, Juliet Jacobsen, and Brad Stuart | 00:51:41 | |
How do people react when they hear they have a serious illness? Shock, “like a car is rushing straight at me” (says Bill Gardner on our podcast). After the shock? Many people strive, struggle, crawl even back toward a “normal” life. And some people, in addition or instead, engage in deep introspection on how to make meaning or live with or understand this experience of serious illness. Today we talk with deep thinkers about this issue. Bill Gardner is a psychologist living with advanced cancer who blogs “I have serious news,” Brad Stuart is an internist and former hospice director whose book is titled, “Facing Death: Spirituality, Science, and Surrender at the End of Life,” and Juliet Jacobson is a palliative care doc who wrote a paper finding that geriatricians do NOT consider aging a serious illness. We have a wide ranging conversation that touches on how to place aging, disability, and multimorbidity in the context of serious illness conversations, “striving toward normal,” stoicism, existentialism, psychedelics, the goals of medicine, medical aid in dying and more. We could have talked for hours! And I get to play a Bob Dylan song that’s been on my bucket list to learn. Enjoy! -@AlexSmithMD
Additional links: Bill Gardner’s article about MAID in Comment Magazine Bill Gardner’s articles about living with terminal cancer in Mockingbird Magazine: https://mbird.com/art/cancer-in-advent/
On how existential threat is stored in the brain.
Papers on “striving toward normalcy” in the setting of serious illness
| |||
| 06 Jul 2023 | How State and Local Agencies on Aging Help Older Adults: A Podcast with Susan DeMarois, Greg Olsen, and Lindsey Yourman | 00:48:59 | |
You may have heard of Area Agencies on Aging, but do you really know what they do or how they do it? What about State Departments of Aging or state master plans for aging? Do you know how these agencies fit in with programs like Meals-on-Wheels or other nutritional support programs? Is your brain hurting yet with all these questions? No? Ok, what about Aging and Disability Resource Connection (ADRC) services? Well, if you are like me, you’ve probably heard of these programs but are at a loss to know exactly what they do. On today's podcast we dive deep into how state and local governments are addressing the needs of older adults, answering all of these questions and more thanks to our three amazing guests: Susan DeMarois (the Director of California Department of Aging), Greg Olsen (the Director of the New York State Office for the Aging), and Lindsey Yourman (the Chief Geriatric Officer for the County of San Diego). It’s a fun podcast with our guest bringing in a ton of knowledge and passion for the work that they do. If there is one take-away from the podcast, it is something Dr. Yourman emailed me after we met: “My hope is that every geriatrics clinician/Geriatrics Department/Division that listens to our podcast will be motivated to reach out to their Area Agency on Aging (if they haven't done so previously) to ask for a meet and greet and to learn about their resources, services, and recommended community-based organizations for older people.” To learn more about what we talked about, check out the following links:
| |||
| 18 Jan 2024 | Substance Use Disorder in Aging and Serious Illness: A Podcast with Katie Fitzgerald Jones, Jessica Merlin, Devon Check | 00:52:28 | |
The CDC’s Guideline for Prescribing Opioids for Chronic Pain excludes those undergoing cancer treatment, palliative care, and end-of-life care. In doing so, it seems to give the impression that pain seen in cancer is inherently different than pain seen in other conditions and that those with cancer may not have the same risk for opioid use disorder as compared to other conditions. Today's podcast tackles these issues and more with three amazing guests: Katie Jones, Jessica Merlin, and Devon Check. We start off the conversation by talking about whether patients with cancer and cancer pain are really that different, and their paper that was just published on January 11th in JAMA Oncology showing that substance use disorder is not uncommon in individuals with cancer. After discussing screening options for substance use disorder, we go on to talk about both the treatments for it and the issues that arise. In particular, we talk about Katie’s and Jesica’s paper in NEJM titled “Juggling Two Full-Time Jobs — Methadone Clinic Engagement and Cancer Care,” which described the difficulty in managing cancer pain and methadone for opioid use disorder. Lastly, we discuss Katie’s paper on substance use disorder in an aging population and how one can incorporate the 5 Ms (ie, matters most, medications, mind, mobility, and multicomplexity) into a framework for age-friendly care for older adults with substance use disorder.
Previous podcasts on substance use disorder
Expert consensus-based guidance
| |||
| 28 Mar 2024 | PC Trials at State of Science: Tom LeBlanc, Kate Courtright, & Corita Grudzen | 00:39:41 | |
One marker of the distance we’ve traveled in palliative care is the blossoming evidence base for the field. Ten years ago we would have been hard pressed to find 3 clinical trial abstracts submitted to the annual meeting, much less high quality randomized trials with robust measures, sample sizes, and analytics plans. Well, as a kick off to this year’s first in-person State of the Science plenary, held in conjunction with the closing Saturday session of the AAHPM/HPNA Annual Assembly, 3 randomized clinical trials were presented. Today we interview the authors of these 3 abstracts about their findings:
Wow! I’m just stunned even writing that! We’ve come so far as a field. This isn’t to say we’ve “made it” - more to say that we’ve reached a new stage of maturation of the field - in which the evidence we are discussing is frequently high quality randomized trial level data. We recorded this on Friday during the annual assembly, and Eric and I were a littttttle off our game due to the residual effects of the GeriPal pub crawl the night before, which were only compounded by technical difficulties. I believe these issues were more than made up for by our guests' forced accompaniment to the song “Feel Like Making Science.” (Credit to the Beeson singing crew for coming up with that one). Enjoy! -@AlexSmithMD
| |||
| 18 May 2023 | AGS Beers Criteria for Potentially Inappropriate Medication Use: A Podcast with Todd Semla and Mike Steinman | 00:45:46 | |
Hot off the press is a brand spanking new updated 2023 AGS Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. The Beers Criteria is one of the most frequently cited reference tools in geriatrics, detailing potentially inappropriate medications to prescribe to older people. We’ve invited two members who helped update the criteria including Todd Semla and Mike Steinman. We discuss a little history of the Beers criteria, including the original Beers Criteria that was published by the late Dr. Mark Beers, and how it has evolved over the last three decades. We also discuss specifics about how to use and not use the Beers Criteria, how medications are selected for inclusion in the criteria, and specifics about certain medications. And of course, take a deep dive by downloading the JAGS paper on the updated Beers Criteria or any of the great links from AGS including the:
| |||
| 28 Apr 2022 | Comics and Humor in Palliative Care: A Podcast with Nathan Gray | 00:44:43 | |
Comics. Cartoons. Graphic Novels. Graphic Medicine. I’m not sure what to title this podcast but I’ve been looking forward to it for some time. Heck, I’m not even sure to call it a podcast, as I think to get the most out of it you should watch it on YouTube. Why, because today we have Nathan Gray joining us. Nathan is a Palliative Care doctor and an assistant professor of Medicine at Johns Hopkins. He uses comics and other artwork to share his experiences in palliative care and educate others about topics like empathy and communication skills. His work has been published in places like the L.A. Times, The BMJ, and Annals of Internal Medicine. We go through a lot of his work, including some of the comics you can see on our blog post. However if you want to take a deeper dive, check out his website “The Ink Vessel” or his amazing twitter feed which has a lot of his work in it.
| |||
| 15 Dec 2022 | Is it time for geriatricians to get on board with lecanemab? Jason Karlawish and Ken Covinsky | 00:49:56 | |
We’ve talked at length on prior podcasts about the failures of aducnumab, Biogen, and the FDA’s decision to approve it. But wait, there’s a shiny new anti-amyloid drug, lecanemab! (No it’s not just the French version of Aducanumab). In an article in the NEJM (a published article this time, wonder of wonders!) lecanemab was shown to slow the rate of cognitive decline by 0.45 points on an 18 point cognitive scale compared to placebo. Wow! Wow? Wait, what? On today’s podcast we talk with Jason Karlawish, who we’ve had on previously talking about his book The Problem of Alzheimer’s and with Aaron Kesselhim, to discuss FDA approval of Aducanumab, as well as frequent guest and host Ken Covinsky. They debate today’s central question: is it time for geriatricians to get on board with lecanemab? Along the way we address:
Their answers may surprise you. As a preview of final thoughts at the end of the episode, Ken and Jason agree that the FDA should approve lecanemab conditional on a post-approval monitoring system and public access to study data, geriatricians should be prepared to have thoughtful conversations with patients about the risks and benefits of lecanemab in view of their values and priorities, and ultimately, that geriatricians should be open to prescribing it. Wow! The times, they are a changin. -@AlexSmithMD | |||
| 18 Feb 2021 | The Problem of Alzheimer's: A Podcast with Jason Karlawish | 00:45:20 | |
Where are we with Alzheimers? Are we about to see a revolution in how we diagnose and treat it with Amyloid PET scans and the amyloid antibody aducanumab (which is currently on FDA’s desk for approval)? Or are we still in the same place where there is no meaningfully effective treatment? Or is it somewhere in between, given the data that we have on comprehensive dementia care? We talk today with Jason Karlawish, a professor of medicine, medical ethics and health policy, and neurology at the University of Pennsylvania Perelman School of Medicine. In addition to being a geriatrician extraordinaire, he is the author of the new book “The Problem of Alzheimer’s: How Science, Culture, and Politics Turned a Rare Disease into a Crisis and What We Can Do About It.” In addition to talking about PET scans and new drugs like aducanumab, we discuss with Jason about the history of Alzheimers, the history of how we care for a fund caregivers, and where we go from here. So take a listen and check out Jason’s book! | |||
| 19 Oct 2023 | POLST Evidence and Update: Kelly Vranas, Abby Dotson, Karl Steinberg, and Scott Halpern | 00:52:02 | |
What level of evidence do we need for POLST to use it ourselves, to advocate for wider usage, and for establishing POLST completion as a quality metric? The answers to these questions will vary. Reasonable people will disagree. And today, on our podcast, our guests disagree. Firmly. AND we are delighted that our guests modeled respectful disagreement. With no hard feelings. Respectful disagreement is in short supply these days. Our guests today are Kelly Vranas, pulm crit care doc who published a systematic review in JAGS of the evidence for POLST (as well as other articles here, here,and here); Abby Dotson, who is Executive Director for National POLST and Director of the Oregon POLST registry; Karl Steinberg, geriatrician and palliative care doc and President of National POLST; and Scott Halpern, pulmonary critical care physician, bioethicists and palliative care researcher who was senior author of a Viewpoint in JAMA that was critical of the concept and evidence base for POLST (and argues little has changed). We had a full podcast, and I wasn’t able to give my take on the existing evidence for POLST, so I’ll write it here. I’m in the middle between Scott and Karl, where I suspect Kelly is, though we didn’t ask her explicitly. On the one hand, I agree with Scott that observational studies finding those who complete a POLST stating a preference for comfort oriented care and DNR are not go to the ICU says little about the effectiveness of POLST. Far more likely that those underlying preferences and values are what drove the findings than completion of the POLST form that codified the preferences into orders. On the other hand, I agree with Karl that the POLST has face validity, and anecdotal evidence is overwhelming. Certainly SOME of those avoided hospitalizations, CPR, and ICU stays were due to documentation of those orders in the POLST. The unanswered question is: HOW MUCH of the differences are due to the POLST? It’s not zero, as many of us have had cases in which we said, “Thank god we completed that POLST, it clearly stopped X from happening.” But is it a tiny, meaningless, fraction? Or a substantial proportion? My guess is a small but meaningful fraction of differences in observational studies is due to completion of the POLST, though the majority of differences are due to underlying preferences and values. Is that fraction due to POLST large enough that we should design quality metrics around completion of POLST? Absolutely not. Do we need better evidence, preferably from an RCT of POLST vs no POLST? Yes. Caveat as well that RCTs should not be placed on pedestal as the only answer- often patients enrolled in RCTs do not represent real world patients - observational studies do. For a trial to have value, it should not exclude patients over age 80, or those with dementia, or patients residing in nursing homes. And it must be powered to detect a small but meaningful difference, not the same level of effect seen in observational studies. OK, I’ll step off my soap box.
Recent JGIM article on POLST in California nursing homes, hospitalization, and nursing home care Karl’s GeriPal post on appropriate use of POLST
-@AlexSmithMD
| |||
| 31 Mar 2022 | Poetry about Aging: Marilyn McEntyre and Guy Micco | 00:42:35 | |
In her essay “Why Read a Poem in a Time Like This?”, Marilyn McEntyre writes: All of us need it. We need it because good poems do something prose can’t do. They invite and enable us to notice the precarious fissures in what we think is solid ground. They direct us toward the light at the edge of things — the horizon, the fragment of dream before dawn, the feeling that’s hard to name, and can only be accurately captured by metaphor. They take us to the edge of “what can’t be said,” and ambush us into feeling before we think, so that we can’t simply and complacently “believe everything we think.” Poetry deals in surprise and subversion and turns old words to new purposes. Marilyn is joined by Guy Micco to talk about why poetry is important in general, why it’s important in medical or nursing education, and why it’s important for people who care for older adults. Along the way, they read poems, talk about poems, and sing a song by John Prine. We talk about how poetry can surprise, how poems can be playful, how they unlock dimensions and emotions that are otherwise locked away. How sometimes good poetry can be like a needed punch. And maybe, just maybe, we convince that poetry skeptic Eric Widera that there is a place for poetry in medicine after all. Enjoy!
Links to essays and books by Marilyn McEntyre
Links to Songs/Poems from the Podcast:
| |||
| 24 Mar 2021 | COVID Vaccine Hesitancy in Frontline Nursing Home Staff | 00:47:43 | |
COVID has taken a devastated toll in nursing homes. Despite representing fewer than 5% of the total US events, at least 40% of COVID‐19–related deaths occurred in older individuals living in nursing homes. The good news is that with the introduction of COVID vaccines in nursing homes, numbers of infections and outbreaks have plummeted. However, only about 2/3rds of nursing home patients and only about ½ of nursing home staff have been vaccinated, largely due to hesitancy about taking the vaccine. On today's podcast we talk about vaccine hesitancy with Sarah Berry, Kimberly Johnson, and David Gifford and the lessons learned from their “town hall” intervention they did that was just published in the Journal of the American Geriatrics Society. A couple of take-home messages for me in this study was that vaccine misinformation was rampant, many nursing staff had lingering questions they wanted answered before getting the shot, and that sharing stories and personal experiences is an important way to overcome hesitancy. In addition to listening to the podcast, we really encourage everyone to take a look at the JAGS article as it has two great tables for anyone willing to do similar town halls. The first is a summary of the concerns of healthcare staff. The second is sample responses to address some of these concerns. | |||
| 14 Jan 2021 | Living with Death: A Podcast with BJ Miller | 00:45:01 | |
Most of us know we are going to die. How often though do we actually let ourselves really internalize that understanding? To imagine it? To feel it? To try to accept it? On today’s podcast we invited BJ Miller back on our podcast to talk about death using as our guide his recent NY Times editorial What Is Death? How the pandemic is changing our understanding of mortality. In addition to being the author of this NY Times article, BJ is a Hospice and Palliative Care doc, and the founder of Mettle Health which aims to provide personalized, holistic consultations for any patient, caregiver or clinician who need help navigating the practical, emotional and existential issues that come with serious illness and disability. We start off with BJ appropriately picking the song "Ebony Eyes" as our intro song, which is a good analogy to talking about death, as it was initially banned by the BBC from airplay as its lyrics were considered too upsetting to play on the radio. We then go into his thoughts on how we picture our deaths and dealing with those emotions we feel when we do, how we “live with death”, and... Also check out BJ’s article that is geared towards kids/students - https://www.nytimes.com/2021/01/06/learning/how-do-you-view-death.html. As BJ put it in an email to us: “It’s fascinating to me how they’re taking care to reach out to younger minds, further proof that the idea that no one wants to think or talk about death - especially youngsters - is bunk. | |||
| 19 Sep 2024 | Stepped Palliative Care: A Podcast with Jennifer Temel, Chris Jones, and Pallavi Kumar | 00:50:17 | |
If palliative care was a drug, one question we would want to know before prescribing it is what dose we should give. Give too little - it may not work. Give too much, it may cause harm (even if the higher dose had no significant side effects, it would require patients to take a lot of unnecessary additional pills as well as increase the cost.) So, what is the effective dose of palliative care? On today’s podcast, we talk about finding an evidence-based answer to this dosing question with three leaders in palliative care: Jennifer Temel, Chris Jones, and Pallavi Kumar. All three of our guests were co-authors of a randomized control trial on “Stepped Palliative Care” published in JAMA this year. We talk about what stepped palliative care is, how it is different from usual care or intensive palliative care, why these palliative care dosing questions are important, and dive deep into the results of their trial. We also discuss some of the other important trials in palliative care, including Jennifer Temel’s landmark NEJM study on outpatient palliative care and another study that gave an intervention we dubbed “fast-food palliative care” in an older GeriPal blog post.
** NOTE: To claim CME credit for this episode, click here **
| |||
| 01 Dec 2023 | Redefining Alzheimer's Disease: A Podcast with Heather Whitson, Jason Karlawish, Lon Schneider | 00:51:31 | |
There is a growing push to change how we define Alzheimer's disease from what was historically a clinically defined syndrome to a newer biological definition based on the presence of positive amyloid biomarkers. This proposed new definition, championed by the Alzheimer's Association (AA) and the National Institute on Aging (NIA), proposes that the disease exists when the earliest manifestation of Alzheimer’s pathophysiology can be detected (amyloid), even though onset of symptoms may be years in the future. On today's podcast we talk about the benefits and drawbacks of redefining Alzheimers to a biological definition with three experts in the disease: Heather Whitson, Jason Karlawish, and Lon Schneider. In particular we spend a good deal of time talking about what this means for asymptomatic patients who may have an abnormal biomarker, which by the proposed new definition would mean they would now have Alzheimer's disease. If you are interested in learning more about the draft guidelines and the response from AGS to these guidelines, check out the following links:
| |||
| 19 Aug 2021 | Loneliness and Social Isolation: Podcast with Carla Perissinotto and Ashwin Kotwal | 00:40:43 | |
“Loneliness is different than isolation and solitude. Loneliness is a subjective feeling where the connections we need are greater than the connections we have. In the gap, we experience loneliness. It’s distinct from the objective state of isolation, which is determined by the number of people around you.” - Vivek Murthy, two time (and current) Surgeon General. We have heard a lot about loneliness and social isolation, particularly during the pandemic with enforced social distancing and near imprisonment of older adults in nursing homes. In this context, we bring in two experts on these topics, Carla Perissinotto and Ashwin Kotwal, to explain:
Some key references from among the many we discuss on the podcast:
-@AlexSmithMD | |||
| 17 Oct 2024 | Guidelines or Goals in Heart Failure: Parag Goyal, Nicole Superville, and Matthew Shuster | 00:48:28 | |
When treating heart failure, how do we distinguish between the expanding list of medications recommended for “Guideline Directed Medical Therapy” (GDMT) and what might be considered runaway polypharmacy? In this week’s podcast, we’ll tackle this crucial question, thanks to a fantastic suggestion from GeriPal listener Matthew Shuster, who will join us as a guest host. We’ve also invited two amazing cardiologists, Parag Goyal and Nicole Superville, to join us about GDMT in heart failure with reduced ejection fraction (HFrEF) and in Heart Failure with preserved EF (HFpEF). We talk about what is heart failure, particularly HFpEF, how we treat it (including the use of sodium–glucose cotransporter-2 inhibitors (SGLT2’s), and how we should apply guidelines to individual patients, especially those with multimorbidity who are taking a lot of other medications. I’d also like to give a shout out to a recent ACP article on HFpEF with an outstanding contribution from Ariela Orkaby, geriatrician extraordinaire (we also just did a podcast with her on frailty).
| |||
| 17 Dec 2020 | Guardianship and End-of-Life Decision Making: A Podcast with Andy Cohen and Liz Dzeng | 00:46:49 | |
Surrogate decision‐making around life-sustaining treatments in the hospital even in the best of circumstances is hard. It’s maybe even harder when caring for those who are conserved or have a professional guardian. The conservator may not have known the patient prior to them losing capacity, they may not know their values or goals that can help guide decisions, and they may be restricted by state statutes on what decisions they can make without getting a judge's approval. The prevailing wisdom is all of the barriers to decision making while under guardianship likely leads to delays in decision making or one that errs on choosing high‐intensity treatment even if it is unlikely to benefit the patient. But is that really the case? On today's podcast, we talk with Andy Cohn, lead author of a recent Journal of the American Geriatrics Society (JAGS) paper titled “Guardianship and End‐of‐Life Care for Veterans with Dementia in Nursing Homes” and Liz Dzeng, the lead author of the accompanying editorial to the paper. The big surprise finding of this study was veterans who were nursing home residents aged 65 and older with moderate to severe dementia and who had a professional guardian were no more likely to receive high‐intensity treatments than the same population who died with decision makers who were not professional guardians. We talk to Andy about his study, potential reasons behind the study, and what, if anything, we should do differently knowing these results. We also talk to Liz about whether substituted judgement is really all that it’s cracked up to be. So take a listen and also check out these articles to read more about it: | |||
| 15 Jul 2021 | Polypharmacy and Deprescribing Super Special: Podcast with Anna Parks, Matthew Growdon, and Mike Steinman | 00:42:00 | |
In a new study in JAGS, Matthew Growdon found that the average number of medications people with dementia took in the outpatient setting was eight, compared to 3 for people without dementia. In another study in JAGS, Anna Parks found that among older adults with atrial fibrillation, less than 10% of disability could be explained by stroke over an almost 8 year time period. She also talked about the need for a new framework for anti-coagulation decisions for patients in the last 6 months of life, based on an article she authored in JAMA Internal Medicine with Ken Covinsky. In today’s podcast we talk with Matthew and Anna, joined by co-author Mike Steinman, to talk about polypharmacy, deprescribing, where we are and what we need to do to stop this freight train of ever more medications for older adults and those living with serious illness. We start by addressing the root cause of the problem. Clinicians want to “do something” to help their patients. And one thing we know how to do is prescribe. It’s much harder psychologically for clinicians to view deprescribing a medication as “doing something.” This attitude needs to change. It will take teamwork to get there, with robust involvement of pharmacists, and likely activating patients to advocate for themselves. And Eric might have mentioned aducanumab a time or two… -AlexSmithMD | |||
| 13 May 2021 | Frailty and Resilience: A Podcast with Linda Fried | 00:39:03 | |
Frailty. What the heck is it? Why does it matter? How do we recognize it and if we do recognize it, is there anything we can do about it? On today’s podcast we talk to Linda Fried, Dean of Columbia University's Mailman School of Public Health and world renown frailty researcher about all things frailty. We talk to Dr. Fried about how she first got interested in frailty, how we define it including the difference between phenotypic frailty and a “deficit accumulation model’ frailty index”, and how we should think about assessing frailty and managing it. We also talk with Dr. Fried about how she thinks about resiliency and the analogy put forth by George A. Kuchel in a wonderful article published in the Journal of American Geriatrics Society (JAGS) that uses the Golden Gate Bridge to explain different definitions of frailty. | |||
| 23 Feb 2023 | Involving the inner circle: Emily Largent, Anne Rohlfing, Lynn Flint & Anne Kelly | 00:46:12 | |
You know when you walk out of a patient's room and have that sense, “This isn’t going to go well.” The patient is sick and getting sicker, and refuses to let you talk with family or other members of her inner circle. Should you stop at “no?” Today we talk with Anne Rohlfing, Lynn Flint, and Anne Kelly, authors of a JGIM article on the reasons we shouldn’t stop at “no.” We owe it to the patient to explore the reasons behind the “no,” commonly not wanting to be a burden to their family. In such cases, we owe it to the patient to use persuasion, for example, “I hear that you don’t want to be a burden. And I’m worried that there may come a time when you have trouble making decisions for yourself. We will have to reach out to your daughter then to help with decisions. Imagine her hearing for the first time that you’re sick, that you’re hospitalized, that you’re in the ICU, and that you can’t make your own decisions? That’s a huge amount of news all at once. It would help her to prepare if we could start talking with her now.” We also talk with Emily Largent, a bioethicist and former ICU nurse, who argues in a Hastings Center Report for an expanded vision of patient consent. Consent is often viewed as “all or nothing” for any specific decision. Emily and colleagues have argued for a wider view of consent that continues to involve patients whose consent may fall in the gray zone - able to express some goals and values, hopes and fears - but not able to think through the complexities of a major decision. I’d hazard that maybe half the patients I care for at the intersection of geriatrics and palliative care fall in the gray zone. Emily’s expanded notion of consent is grounded in the concept of “relational autonomy.” Relational autonomy was was first introduced to bioethics by feminist scholars, who observed that most people do not make decisions as isolated islands. Rather, most of us live and make decisions in relationship to one another. Emily’s notion also borrows from pediatric bioethics, in which parents can look to young children for assent and input on decisions, empowering them to some extent. Invoking this principle, Emily argues for an expanded role for patients in the gray area and their inner circle working together along a spectrum of cooperative decision-making. My favorite line from Emily’s paper: “Geriatric assent has not been widely adopted in clinical care, but bioethicists should advocate for this, as adoption of partial-involvement strategies can prolong the period in which individuals are (appropriately) engaged in decisions about their health care.” Enjoy! -@AlexSmithMD
| |||
| 19 May 2022 | Rethinking Opioid Conversions: Mary Lynn McPherson and Drew Rosielle | 00:50:58 | |
A patient is on morphine and you want to convert it to another opioid like hydromorphone (dilaudid). How do you do that? Do you do what I do, pull out a handy-dandy opioid equianalgesic table to give you a guide on how much to convert to? Well on today’s podcast we invited Drew Rosielle on our podcast who published this Pallimed post about why opioid equianalgesic tables are broken and why we shouldn't use them, as well as what we need to move to instead. But wait, before you throw out that equianalgesic table, we also invited Dr. Mary Lynn McPherson, PharmD extraordinaire who published this amazing book, Demystifying Opioid Conversions, 2nd Ed., which advocates for an updated, wait for it… equianalgesic table! Oh boy, what should we do? Should we throw out the equianalgesic table like some are advocating we do with advance directives (see here), or should we just modernize it for the times with updated data? Listen to this spicy podcast with these wonderful guests to make up your own minds (I’m sticking with the equianalgesic table for now). If you want to take a deeper dive into some of the references, here you go:
| |||
| 21 Oct 2021 | “Real world” eligibility for aducanumab: A Podcast with Tim Anderson and Marco Canevelli | 00:46:28 | |
The FDA label for the amyloid antibody aducanumab (Aduhelm) started off exceedingly broad, basically including anyone with Alzheimer's disease, but was subsequently narrowed to to patients with mild cognitive impairment (MCI) or mild dementia due to Alzheimer disease (AD). Should, though, the label be even more restrictive to mirror the populations studied in the two still unpublished trials of the drug, EMERGE and ENGAGE? Or should CMS consider restricting coverage for aducanumab to populations meeting trial eligibility criteria and requiring additional evidence on clinical outcomes in groups excluded from the trials? In today's podcast, we talk with Tim Anderson and Marco Canevelli, the authors of two recent articles published about the real world eligibility of aducanumab: Tim Anderson was first author of a JAMA research letter that found that more than 92% of Medicare beneficiaries with Alzheimer's Dementia and 85% of those with MCI would have been excluded in the clinical trials of aducanumab based on their age or comorbid conditions. Marco was first author of a JAGS letter to the editor that systematically applied the EMERGE and ENGAGE exclusions to 911 patients with cognitive complaints who went to A geriatric outpatient unit in Milan (Italy). Only six patients (i.e., 0.66%) of these patients would potentially be candidates to aducanumab. For more podcasts on aducanumab, check out these two: | |||
| 10 Oct 2024 | Intentionally Interprofessional Care: DorAnne Donesky, Michelle Milic, Naomi Saks, & Cara Wallace | 00:47:56 | |
In fellowship, one of the leaders at MGH used to quote Balfour Mount as saying, “You say you’ve worked on teams? Show me your scars.” Scars, really? Yes. I’ve been there. You probably have too. On the one hand, I don’t think interprofessional teamwork needs to be scarring. On the other hand, though it goes against my middle-child “can’t we all get along” nature, disagreement is a key aspect of high functioning teams. The key is to foster an environment of curiosity and humility that welcomes and even encourages a diversity of perspectives, including direct disagreement. Today we talk with DorAnne Donesky, Michelle Milic, Naomi Saks, & Cara Wallace about the notion that we should revolutionize our education programs, training programs, teams, incentive structures, and practice to be intentionally interprofessional in all phases. The many arguments, theories, & approaches across settings and conditions are explored in detail in the book they edited, “Intentionally Interprofessional Palliative Care” (discount code AMPROMD9). Of note: these lessons apply to geriatrics, primary care, hospital medicine, critical care, cancer care, etc, etc. And they begin on today’s podcast with one clinical ask: everyone should be a generalist and a specialist. In other words, in addition to being a specialist (e.g. social worker, chaplain), everyone should be able to ask a question or two about spiritual concerns, social concerns, or physical concerns. Many more approaches to being interprofessional on today’s podcast. But how about you! What will you commit to in order to be more intentionally interprofessional? If we build this dream together, standing strong forever, nothing’s gonna stop us now… -@AlexSmithMD
Interprofessional organizations that are not specific to palliative care are doing excellent work
This episode of the GeriPal Podcast is sponsored by UCSF’s Division of Palliative Medicine, an amazing group doing world-class palliative care. They are looking to build on both their research and clinical programs and are interviewing candidates for the Associate Chief of Research and for full-time physician faculty to join them in the inpatient and outpatient setting. To learn more about job opportunities, please click here: https://
** NOTE: To claim CME credit for this episode, click here ** | |||
| 11 Jul 2024 | Palliative Care in Liver Disease: A Podcast with Kirsten Engel, Sarah Gillespie-Heyman, Brittany Waterman, & Amy Johnson | 00:51:24 | |
In May we did a podcast on KidneyPal (the integration of palliative care in renal disease), which made us think, hmmm… one organ right next door is the liver. Maybe we should do a podcast on LiverPal? (or should we call it HepatoPal?) On today’s podcast, we do that by inviting four palliative care leaders who are integrating palliative care into the care of those with liver disease: Kirsten Engel, Sarah Gillespie-Heyman, Brittany Waterman, and Amy Johnson. It’s a jampacked 50 minutes, filled with pearls on taking care of patients with liver disease. We cover:
Also, if you want to take an ever deeper dive, check out our 2022 podcast on End Stage Liver Disease with Jen Lai, Ricky Shinall, Nneka Ufere, and Arpan Patel
| |||
| 01 Jul 2021 | Race/ethnic differences in end-of-life care: Podcast with Rashmi Sharma and Zhi Jia | 00:47:15 | |
We have made remarkable progress in reducing the use of feeding tubes for patients with advanced dementia. This has been due to the leadership of people like Susan Mitchell and Joan Teno, among others. One might hope that this reduction in use of feeding tubes has been in part due to advance care planning discussions that helped align care and treatment with patients goals. How then, do we explain the concerning findings in a pair of recent papers demonstrating high rates of mechanical ventilation among patients with dementia? In today’s podcast, we talk with Rashmi Sharma, who in JAGS found that rates of mechanical ventilation rose from 4% to 12% among whites with advanced dementia and 9% to 22% among blacks between 2001 and 2014. One in five blacks with advanced dementia admitted from a nursing home received mechanical ventilation. That’s startling. And Zhi Jia found in a Medicare sample that Asians were more likely to receive mechanical ventilation than whites, and disparities were higher for older Asians with dementia compared to cancer. We have made progress, due to the leadership of GeriPal superstars. But even as we make progress in feeding tubes, it doesn’t seem to have translated across the board to mechanical ventilation, a burdensome and potentially non-beneficial treatment for patients with dementia. The fact that rates are highest among older blacks and Asians is particularly concerning. Though the reasons behind this are complex, it’s likely that structural racism plays a major role in these growing inequalities. We have more work to do.
| |||
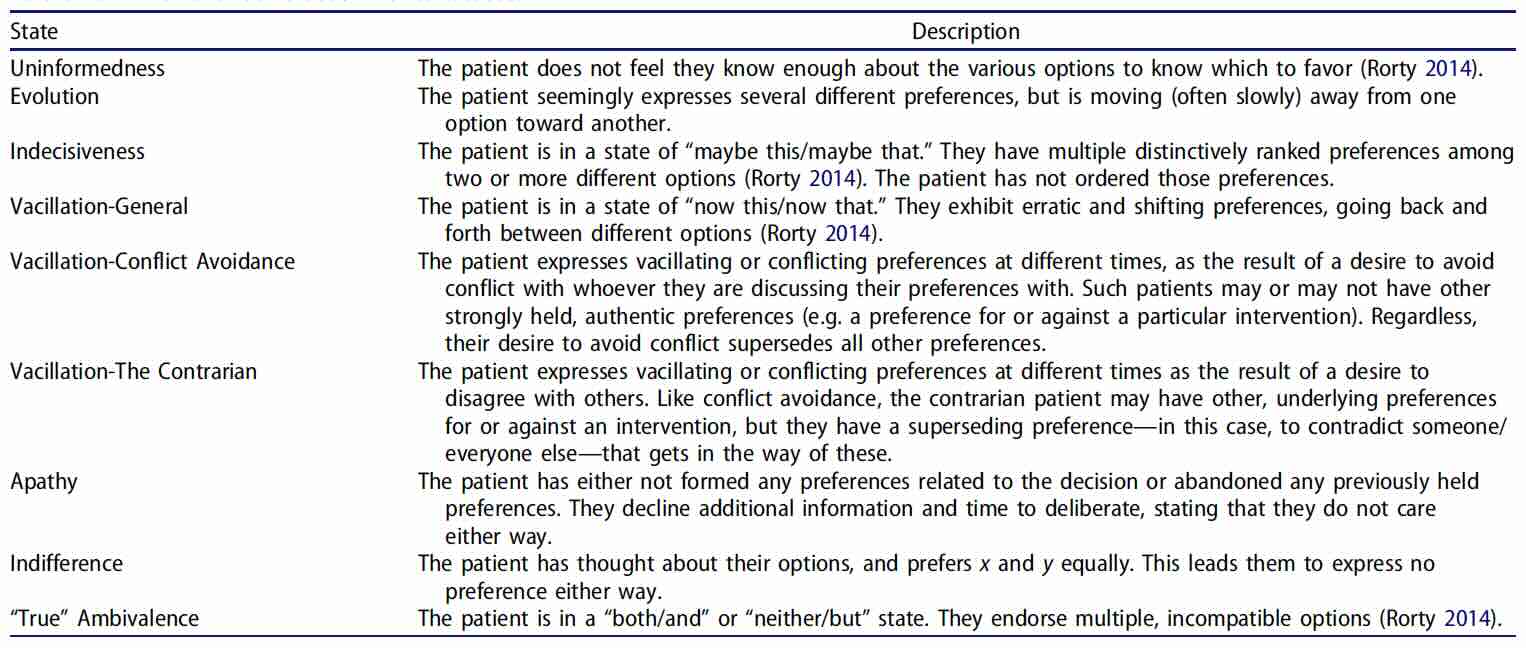



{kind=link}